 Newsletter
NewsletterAn overview of the clinical ramifications of various curing lights will help clinicians make the right choice for their practice.
By Leendert (Len) Boksman, DDS, BSc, FADI, FICD | Gildo Coelho Santos, Jr., DDS, MSc, PhD
The use of bonded restorations in restorative dentistry continues to increase, including the number of resin-based composite restorations placed instead of amalgam.1 Factors that may affect polymerization of resin-based composite restorations include light intensity, exposure time, and wavelength as related to the type of photoinitiator incorporated in the resin-based composite material.
More than 37% of composite restorations are clinically insufficiently cured, and most of the time it is due to light-curing units with intensities of less than 300 mW/cm2, which are described in the dental literature as inadequate, unusable, or unsuitable.2 Three international studies conducted to measure the intensity of light-curing units used for polymerization of resin composites in private dental offices reported that 33% to 48% of the lights in dental offices had intensities of less than 300 mW/cm2.2-4
Clinicians must understand the principles of light-curing because unbound monomers are cytotoxic. As well, under-curing can cause flex with pumping of the restoration, resulting in postoperative sensitivity.5The effectiveness of a light-curing procedure depends on the light’s output power as well as its light spectrum and tip design. The curing exposure time, resin chemistry, photoinitiator type, location and orientation of the restoration, materials that partially block the light, and the clinician’s ability to aim and maintain the light on or at the target at 90 degrees are also important factors.6 The spectrum of light used with light-cured dental composite materials ranges from about 380 nm to 500 nm, with camphorquinone being the most common photo-absorbing initiator. These photo-initiators absorb photon energy and react with the amine activator, creating free radicals that initiate polymerization. Camphorquinone, which has its major absorption at about 470 nm, is yellow in color. Therefore, glazes, very light-colored composites, incisal shades, and translucent shades may contain other initiators such as phenyl-propanedione (PPD) and Lucirin TPO, which have their highest absorption below 400 nm.7
Quartz Tungsten Halogen (QTH) Lights
These lights contain an incandescent lamp with a tungsten filament in an inert gas with a small amount of halogen. An electric current heats the tungsten to 2727°C, creating visible light and infrared radiation, which is absorbed by the composite and results in great molecular vibration and generation of heat.8 This heat generation necessitates fan cooling, which may be noisy and result in a bioburden trap. The light is filtered to approximately 390 nm to 500 nm, which is capable of curing all composites, but the challenge with these lights is that they only use 9% of the total energy produced, with a bulb life of approximately 30 to 50 hours before they start to denature and need to be replaced. The filter can accumulate dust, crack, or delaminate, which can alter the wavelengths of light transmitted, allowing harmful UV rays to be emitted. Also, narrow light tips emit a small curing footprint, which can necessitate multiple curing cycles in large restorations.
Plasma Arc Lights
These lights have a bulb that is an aluminum oxide high-pressure vessel that contains highly pressurized xenon gas under 150 psi. The inside shape is specified to reflect light between two electrodes and the arc is about 1 mm long, enabling a very focused beam. The challenges of this light include high infrared and ultraviolet emission and a large sink radiator to strip off the extreme heat produced by these lamps. The replacement bulbs can cost up to $600. The base units are large and the unit may require a cord that is liquid-filled, which may deteriorate over time. These expensive lights may not cure all photo-initiators and the narrow light guides emit a small curing footprint.
Argon Laser Lights
This type of unit generates light when energy is applied to an atom, raising an electron to a higher, unstable energy level. The electron will return to a stable level by releasing light through a medium of argon gas. These lights have large, heavy base units that not very portable. The tips are small, making multiple cure cycles necessary. Fast curing can cause a large temperature increase and considerable shrinkage stress, which can result in postoperative sensitivity issues. These lights may not cure all composite materials, and they are expensive.
Light-Emission Diode (LED) Curing Lights
LED curing lights have gone through multiple generations. The first generation had a narrow emission spectrum that could activate camphorquinone but not other photo-initiators, and thus could not fully polymerize some composite materials. Their power and energy output was low, necessitating long curing times for a complete cure.9 The light tips had a small footprint, and the lights had an insufficient continuous operation before shutdown. The second generation of LED curing lights have a higher photon energy output. However, they have a one-color chip with a narrow emission spectrum that does not cure all composites. Many are cordless, and all batteries have a limited life expectancy, and are expensive to replace. Some have fans that are noisy and can be a bioburden trap, with the light tips subject to easy breakage. Many of these lights have the limitation of being insufficient for continuous operation, such as would be needed for cementing multiple crown-and-bridge units or veneers.10
The ideal light-curing unit should have a broad emission spectrum, sufficient light intensity, minimal drop off of energy with distance, multiple curing modes, sufficient duration for multiple curing cycles, durability, a large curing footprint, and be easily repairable.
The objective is sufficient polymerization, and so the light needs to be collimated, which is critical for focusing the light at greater distances. Increased light exposure ensures increased depth of cure, increased conversion or polymerization, and increased hardness. Inadequate light intensity or energy leads to inadequate polymerization and increased bacterial colonization, which can reduce bond strength, decrease retention, and result in inferior physical properties, excessive wear, bulk fracture, color instability, and increased microleakage, which in turn will result in secondary caries, staining, and postoperative sensitivity.11
One must remember that when light intensity is measured by itself at a specific depth, this has no correlation to what happens when a composite is placed at that depth, because, as the light passes through composite, the light is attenuated drastically depending on the filler type, filler loading, hue of the composite, refractive properties, opacity, and translucency.12
In order to decide how long it takes to adequately cure a composite, one has to look at the energy density used, which is the irradiance of the light multiplied by the time of application (measured in Joules). The distance from the composite surface drastically affects the power generated. The collimation of the light, or how much light is wasted when not focused forward, can drastically affect the power at depth (Figure 1). As mentioned earlier, the wavelengths and the type of composite affect the efficiency of light-curing. The bottom line is that it takes about 17 J/cm2 to 20 J/cm2, which equates to 20 seconds with a 1,000-mW/cm2 light energy to obtain the optimum degree of polymerization of a composite. Independent of the technique being used and the care the clinician takes during the process, insufficient irradiance can lead to inadequate polymerization even after the recommended curing times. We know that turbo tips that channel the light suffer from poor energy at distance and in unique situations, such as very deep cavity preparations, trans-tooth curing, opaque composites, or the curing of resin cements through indirect ceramic veneers, onlays, or crowns. For these cases, increased curing time is mandatory (Figure 2).13
The new multi-spectrum LED lights emit energy at the absorption spectrum for camphorquinone, Lucirin TPO, and phenylpropanedione, thus curing all composites14 and are the current state-of-the-art for clinical practice. However, the current market selection is limited. In the desired category of broadband curing lights, VALO (Ultradent Products Inc., www.ultradent.com) with its patented technology delivers more power than any other curing light.15 It uses a thermally conductive layer to distribute heat from the LED to the aluminum body of the curing light, eliminating the need for a cooling fan. Using highly efficient LEDs with a thermal management system that drives the chip at only 30% of its available capacity, the chip runs substantially cool, while maintaining consistent performance even in the most challenging and demanding curing needs. The light has four LED curing chips with a range of 395 nm to 480 nm, thus effectively curing all composites (Figure 3). The light has rhodium-coated reflectors that ensure better collimation of the light, and an internal glass lens that will not discolor to affect light transmission, nor create heat generation due to reflection. VALO produces a more uniform and larger area of curing than any of the other broadband lights (Figure 4). The standard mode of 1,000 mW/cm2 has 5-, 10-, 15-, and 20-second curing cycle times, with the high-power tack mode at 1,400 mW/cm2 having curing times of 1, 2, 3, and 4 seconds.
The Xtra Power or Plasma Emulation mode has a power output that exceeds 3,200 mW/cm2, with a curing time of 3 seconds. The corded light goes to sleep after 1 hour of inactivity and the cordless after 60 to 90 seconds. Reactivation occurs by pressing any button returning it to the last setting used or simply touching the unit to activate the motion sensor for the battery-operated unit. VALO loses approximately 40% of its energy at 10 mm, while most lights lose between 60% to 80% of their power at 10 mm (Figure 5).16 Therefore, it is imperative that at distance, the curing time is increased to compensate. The distance between the tip of the light guide and the cavity floor of a typical Class II preparation was reported by Price to be in the range of 6.3 mm with a standard deviation of 0.7 mm in 15% of restorations deeper than 8 mm.17 Of course, this distance can be increased when separation rings or matrices get in the way of the light tip (Figure 6). The more collimated or channeled a light is, the less it diverges and spreads as it is moved away from the area to be cured, so more energy is available at depth. A 90° placement angle is critical for depth penetration of the light energy, which falls off drastically as the light is held at an angle to the restoration (Figure 7 and Figure 8). Some clinicians only deliver 20% of the energy achieved by other clinicians using the same curing light at the same location because they fail to place the light as close to the restoration at 90°. Price et al demonstrated that VALO produces the highest degree of conversion or polymerization of any lights tested.18 A higher degree of conversion produces higher hardness values. The low 5° profile of VALO not only assures adequate access to the cavity preparation no matter where it is orally, but also ensures that a 90° angle is easily maintained for the best curing penetration. Many glass curing tips are angled 35° to 50°, making it impossible to attain the 90° angle intraorally especially in posterior Class II restorations (Figure 9). The VALO body is created with an extremely hard sapphire coating that has been Teflon-impregnated for less bioburden accumulation and easy cleaning. The 9.8-mm scratch-resistant glass lens is easily cleaned, and the tip is virtually indestructible versus the fragile long glass curing tips of other lights. For the cordless version, the batteries are the lowest cost of any curing light in the dental marketplace.
Other broadband curing lights include the bluephase 20i (Ivoclar Vivadent, ivoclarvivadent.com), which has two color chips, and a light output between 1,200 mW/cm2 and 2,000 mW/cm2, as well as a low-power and soft-start mode. This light also has an integrated cooling fan without side slots, eliminating the potential bioburden problem. Another multispectrum curing light is the SmartLite® Max (DENTSPLY Caulk, www.) with dual LEDs and a 1,200-mW/cm2 output that can be boosted to 1,400 mW/cm2.
Clinicians currently have few choices in the broadband light category for curing dental composite restorations. Careful evaluation of the requirements for the wide variation in light curing applications and material variations should make the choice easy.
The authors received material support from Ultradent Products, Inc., for writing this article.
1. Eklund SA. Trends in dental treatment 1992 to 2007. J Am Dent Assoc. 2010;141(4):391-399.
2. El-Mowafy OM, El-Badrawy WA, Lewis DW, et al. Intensity of quartz-tungsten-halogen light-curing units used in private practice in Toronto. J Am Dent Assoc. 2005;136:766-773.
3. Santos Jr GC, Coelho Santos MJM, El-Mowafy OM, El-Badrawy W. Light intensity of quartz-tungsten-halogen light polymerization units used in dental offices in Brazil. Int J Prosthodont. 2005;18(5):151-152.
4. El-Mowafy O, El-Badrawy W, Lewis DW, et al. Efficacy of halogen photopolymerization units in private dental offices in Toronto. J Can Dent Assoc. 2005;71(8):587.
5. Uhl A, Volpel A, Sigusch BW. Influence of light curing units and dental composite polymerization on cells in vitro.J Dent. 2006;34(4):298-306.
6. Christensen GJ. Save time, effort and money with fast, new LED curing lights. Clinicians Report. 2010;3(10):1-3.
7. Price RBT, Felix CA. Effect of delivering light in specific narrow bandwidths from 394-515 nm on the micro-hardness of resin composites. Dent Mater. 2009;25(7):899-908.
8. Uhl A, Mills RW, Jandt KD. Polymerization and light-induced heat of dental composites cured with LED and halogen technology. Biomaterials. 2003;24(10):1809-1820.
9. Uhl A, Mills RW, Jandt KD. Photoinitiator dependent composite depth of cure and Knoop hardness with halogen and LED light curing units. Biomaterials. 2003;24:1787-1795.
10. American Dental Association. ADA Professional Product Review. Curing Lights. 2009;4(4).
11. Mahn E. Light polymerization. Inside Dentistry. 2011;7(2):66-71.
12. Hervás-García A, Martínez-Lozano MA, Cabanes-Vila J, et al. Composite resins. A review of the materials and clinical indications. Med Oral Patol Oral Cir Bucal. 2006;11:E215-E220.
13. Corciolani G, Vichi A, Swift EJ. Turbo tips. J Esthet Restor Dent. 2011;23(5):294-295.
14. Swift Jr EJ. Critical appraisal: Light curing. J Esthet Restor Dent. 2011;23(3):191-196.
15. Price RBT, Felix CM, Whalen JM. Factors affecting the energy delivered to simulated Class I and Class V preparations. J Can Dent Assoc. 2010;76(a94):1-12.
16. Felix CA, Price R. The effect of distance from light source on light intensity from curing lights. J Adhes Dent. 2003;5(4):283-291.
17. Hansen EK, Asmussen E. Visible-light curing units: correlation between depth of cure and distance between exit window and resin surface. Acta Odontol Scand. 1997;55:162-166.
18. Price RBT, Felix CA, Andreou P. Third-generation vs. a second-generation LED curing light: Effect on Knoop Hardness. Compend Contin Educ Dent. 2006;27(9):490-497.
Leendert (Len) Boksman, DDS, BSc, FADI, FICD
Retired from Private Practice
London, Ontario, Canada
Gildo Coelho Santos, Jr., DDS, MSc, PhD
Assistant Professor and Chair Division of Restorative Dentistry
Schulich School of Medicine and Dentistry
University of Western Ontario
London, Ontario, Canada
Private Practice
London, Ontario, Canada
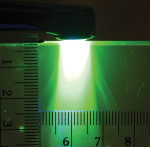
Figure 1
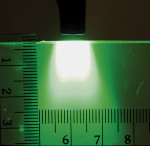
Figure 2
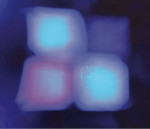
Figure 3

Figure 4
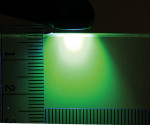
Figure 5

Figure 6

Figure 7
Figure 8

Fig












