 Newsletter
NewsletterNew materials simplify the process.
By Todd C. Snyder, DDS, AAACD
Those who have not yet switched to a digital impression-capturing device still are likely to be using impression materials for many of the everyday indirectly fabricated procedures performed in the dental office. The ability to create an accurate reproduction of teeth using a dimensionally stable impression material has been sought for many years. The need for an impression material to provide a precise, accurate reproduction of soft tissues, teeth, and dental restorations—all within a wet environment—is a necessity for most dental healthcare professionals. There are numerous options available for taking impressions—hydrocolloids, polyethers, polyvinyls, polyether/polyvinyl blends, and digital impression devices. Modern technology and science allow dental materials to continue to evolve and improve, coming closer to having ideal characteristics that can overcome many of the daily shortcomings of current materials. This case demonstrates how some new materials may be making the impression process easier than ever before.
Impression and Over-Impression Method
In this case, the patient presented with a missing restoration on the lower left first molar (tooth No. 19) (Figure 1). Additionally, tooth No. 18 had a fractured mesial root that required extraction because it was non-restorable (Figure 2). The patient was anesthetized using a compounded topical (Inland Compounding Pharmacy, www.inlandcompounding.com) followed by a single carpule of buffered 2% lidocaine with 1:100,000 epinephrine using the OnSet® system (OnPharma®, www.onpharma.com).
The absence of a restoration in tooth No. 19 required a replacement material to mimic the necessary occlusion and tooth structure. A pseudo filling/mock-up was placed to recreate the anatomical shape and occlusion so that an over-impression could be fabricated to facilitate the provisionalization process upon completion of the final tooth preparation. The tooth was built up to ideal shape and size without the use of a traditional bonding agent. The direct composite restorative material (Premise, Kerr Corporation, www.kerrdental.com) was placed only momentarily as a temporary full-contour restoration.
After adapting the material to the cavosurface margin of the tooth, it was then adjusted against the adjacent premolar (tooth No. 20) to create an interproximal contact. Next, the patient was instructed to bite down to facilitate the creation of the occlusal anatomy and functional stops on the tooth. After this was completed, any additional composite material was either removed or adapted to the tooth, followed by 10 seconds of light-curing of the composite material. This temporarily placed material was a working prototype to allow for the creation of the ideal occlusion and shape to be created in the provisional.
An over-impression was then taken of the pseudo filling/mock-up restoration using a fast-setting bite registration material (Futar® Bite Registration Material, Kettenbach LP, www.kettenbachusa.com) and a quadrant impression tray (HEATWAVE™, Clinician’s Choice® Dental Products, www.clinicianschoice.com) to facilitate making a provisional later after completing the indirect restoration preparation. The over-impression was set aside, and the composite material that had been placed in the tooth defect was easily removed from the tooth with a spoon excavator because a bonding agent was not used and an incomplete curing cycle was performed. A retraction cord (#00 Ultradent, Ultradent Products, Inc., www.ultradent.com) was then placed around the tooth to facilitate gingival tissue displacement, creating space for the impression material.
The Panasil® Binetics Putty Soft (Kettenbach) was dispensed from the automix machine directly into the impression tray while the Panasil® Initial Contact Light syringe material was simultaneously dispensed around the tooth and onto the adjacent teeth. The whole time the wash was being applied to tooth No. 19, the tip of the impression material was kept in the material to avoid incorporating any voids. The tray was seated onto the light-body wash encompassing the teeth. The Panasil® Binetics Heavy Putty’s high viscosity provides ample pressure, which can force the light-body wash down around the teeth and into the sulcus.
Upon removing the impression, it quickly became apparent that the hydrophilicity and hydrostatic pressure of the heavy-body putty and use of a non-perforated, solid impression tray allowed for the light-body material to have been driven down the fractured root, even in the presence of moisture in this unusually challenging location, as tooth No. 18 was not able to be dried significantly before taking the impression of tooth No. 19 (Figure 3). The fracture that was present on No. 18 was not very large, and the two sections of tooth structure were not mobile. Of note, the material had extended approximately 11 mm down the cracked root (Figure 4); in addition, the excellent adaptation and high tear strength enabled the Panasil® light-body impression material to be removed in one piece from inside the cracked root.
Restoration Fabrication
The provisional restoration was fabricated next from the over-impression that was created at the beginning of the appointment. The provisional material (Fill-In, Kerr Corporation) was syringed into the over-impression, filling only tooth No. 19 about two thirds full. The over-impression was then placed onto the teeth in the mouth for 1 minute. The over-impression was then removed, leaving the new provisional intact within the impression. It was subsequently removed from the over-impression and trimmed, polished, and tried back onto the tooth. The mesial contact was checked for tightness with floss, followed by occlusal equilibration using both Shimstock Occlusion Foil (Almore International, Inc., www.almore.com) for bite pressure and Troll foil (TrollDental, http://trolldental.com) for delineating occlusal contacts (Figure 5).
The provisional restoration was cemented using Cling 2 provisional cement (Clinician’s Choice). A thin bead of temporary cement was placed just along the margin of the provisional so that complete seating of the restoration as well as sealing of the margin could be obtained. This assists in not having to adjust occlusion on the provisional from incomplete seating due to overfilling the provisional cement with film thickness and viscosity typically not allowing for complete seating. Tooth No. 18 was subsequently extracted without any complications.
When the patient returned for the try-in appointment, the provisional was removed followed by cleansing of the tooth structure. The gold restoration was tried in and evaluated for marginal adaptation, contacts, and occlusion.2 With no adjustments being necessary, the restoration was then cemented with Ceramir® Crown & Bridge Bioceramic Luting Cement (Doxa Dental Inc., www.ceramirUS.com) (Figure 6).3,4
The ability to quickly capture an accurate impression of teeth with an impression material is becoming easier, thanks in part to companies like Kettenbach with their new line of impression materials. The Panasil® product line by Kettenbach includes both extra-light and light-body wash materials that come in either fast-set (2 minutes) or regular-set times (2 minutes, 30 seconds) (Figure 7).1 Panasil® Putty is one of only two materials on the market packaged for use in the automix machines. The unique Panasil® Binetics Putty also comes in a fast set as well as a regular set. A key feature with this product line is that it starts to set on initial contact, so the amount of time the product is in the mouth is actually lessened, while still providing sufficient working time as dictated for the clinical case. Other reasons to try these products include the following:
• Kettenbach has one of the broadest selections of impression material options available—in essence, a viscosity and a set time that meets an individual practice’s needs.
• Patented hydrophilicity technology provides a very low contact-wetting angle (Figure 8).
• As a direct seller, Kettenbach has successfully kept material costs lower than other popularly used brands.
• Highly thixotropic materials flow only under pressure, which puts the clinician in control.
• Attractive low-cost starter programs are backed by unconditional guarantees, enabling clinicians to buy the product only if they are satisfied.
• Products are highly acclaimed by multiple rating agencies, such as Dental Advisor, Reality, and Clinical Research Associates.
Todd C. Snyder, DDS, AAACD
Private Practice
Laguna Niguel, California

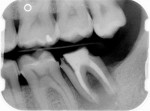
Figure 1 Figure 2 Figure 3
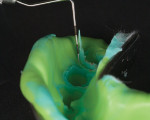

Figure 4 Figure 5 Figure 6

Figure 7 Figure 8















