Newsletter
NewsletterSingle-visit customized anterior ceramics are made possible with CAD/CAM technology.
By Brent Harris, DMD
For a majority of dentists, one of the biggest esthetic challenges is to fabricate a single maxillary incisor that blends harmoniously with adjacent non-restored teeth. In many cases, patients are advised to restore multiple teeth to ensure continuity of color, or accept that the restorative process may take a number of weeks and involve multiple try-in visits to achieve the desired result. With CAD/CAM dental technology becoming increasing popular, patients are be coming accustomed to completing the entire restorative process in one visit. Often, however, these same-day restorations are limited to the posterior teeth, with challenging anterior cases being fielded out to the laboratory or relegated to a multi-phased visit. With proper treatment planning, a detailed color and contour map of the involved teeth, and the dynamic characteristics of the CAD/CAM software and ceramics available, it is feasible to achieve anterior functional and esthetic excellence in a single visit.
A 66-year-old female patient presented with a horizontally fractured right maxillary lateral incisor sustained as a result of a fall (Figure 1). Clinically, the fracture appeared to be limited to the enamel and dentin of tooth No. 7, and both central incisors showed vertical and horizontal craze lines that were not as prominent prior to the trauma. The patient had already been cleared for any potential bony fractures of the maxilla; however, the entire maxillary anterior segment was exceptionally hypersensitive and tender to palpation and percussion. The fractured incisal portion of tooth No. 7 had been retrieved and rinsed free of debris in distilled water by the patient.
In order to immediately repair the tooth in the most efficient and conservative manner possible, the tooth fragment was initially bonded back into position using a flowable composite resin (Figure 2). The patient’s occlusion was adjusted slightly to minimize working and nonworking contacts on the fractured tooth. During the weeks following the trauma, the patient was happy with the esthetics of the repair on tooth No. 7 (Figure 3); however, she did notice a slight increase in cervical warmth of color on teeth Nos. 7 and 8. Eight weeks after the initial bonding procedure, the patient returned with the tooth fragment fractured off again. After a thorough discussion of treatment options, the patient decided to proceed with fabrication of an all-ceramic crown to restore tooth No. 7. The tooth fragment was once again bonded back into position, this time using Multilink® Automix resin cement (Ivoclar Vivadent), and the patient reappointed for her restorative visit.
It is entirely possible that with the right restorative materials and techniques, along with a thorough occlusal evaluation, this patient may have been able to be definitively treated with conservative bonding of the fractured tooth fragment into place. However, the patient was concerned it would fracture again, leaving her with an esthetic dilemma. A detailed discussion of restorative material choices and techniques ensued. The patient chose the technology and efficiency of a same day CAD/CAM procedure using the E4D Dentist system (D4D Technologies, www.e4d.com) and IPS e.max® CAD lithium disilicate glass-ceramic (Ivoclar Vivadent, www.ivoclarvivadent.com).
Digital photographs were taken to analyze the contour, texture, and color of the adjacent dentition, and to help determine the shade of the e.max ceramic blocks necessary. By photographing and analyzing characteristics such as base shade, translucency levels, areas of high and low chroma/value, and textures, a predictable color/contour map was devised that served as a blueprint for customizing the final ceramic restoration (Figure 4).
When examining the contour of tooth No. 7, it was important to consider the shape and texture of teeth Nos. 6, 8, 9, and 10. Specifically, it was noted that the incisal embrasure created by the mesio and disto-incisal corners of tooth No. 10 were drastically different. The mesio-incisal corner of tooth No. 10 came to a sharp point with a prominent mesio-facial line angle emanating from it. When viewed from the direct facial, this produced a significant linear reflection of light that needed to be duplicated on the restoration for tooth No. 7. The distal contours of tooth No. 10 were much more rounded and wrapped palatally, allowing the canine distal to it (tooth No. 11) to appear more prominent mesio-facially. More light was absorbed on the rounded distal aspect of the left lateral incisor, creating a lower value, shadow-like translucency. All of the maxillary anteriors showed prominent vertical striations, with cervically positioned horizontal striations. The reflection of light off the central incisors showed mid-facial horizontal grooves, while the lateral incisor and canine (teeth Nos. 10 and 11) showed a light reflection consistent with slight dimpling around the cervical region.
From a color standpoint, two notable factors regarding the anterior teeth were imperative to duplicate in order to blend the restoration into the natural dentition. First, the low value translucency of the incisal and line-angle surfaces in comparison to the higher value mid-tooth and cervical regions would have made a monochromatic crown stand out unnaturally. Secondly, the white striation patterns that crisscross the adjacent teeth created a subtle but noticeable geometry, which if not duplicated would have immediately drawn the eye to the lateral incisor restoration.
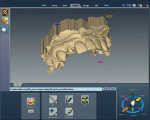
On the preparation day, the patient presented with the fragment from tooth No. 7 still successfully bonded in place. The maxillary anterior teeth were scanned as “clones” intraorally using the E4D Dentist. The scan was verified on the computer and appeared to have stitched together accurately (Figure 5). The maxillary right lateral incisor was then prepared for a full-ceramic crown with deep chamfer/shoulder margins to allow for a full 2 mm of ceramic thickness. A slightly more aggressive preparation was done to prevent the restoration’s color from becoming compromised if the tooth stump became discolored over time as a result of the traumatic incident. Retraction around tooth No. 7 was achieved with a double retraction cord technique, allowing the anterior maxillary teeth and preparation to be scanned intraorally (Figure 6). A single-tooth bite registration was made and scanned intraorally as well. Using E4D’s CAD software, a detailed proposal was generated based on the scanned preoperative clone. The design proposal was refined using the CAD software and the bite was verified using the scanned bite registration (Figure 7). An e.max Low Translucency (LT) ceramic block was chosen and the block shades were narrowed down to A1and B1. In this case, both shades of blocks were milled to clinically compare colors and achieve the closest base color match possible. Both milled restorations were tried in the mouth prior to crystallization to ensure proper fit, contacts, occlusion, and contour. Using the mapping of characteristics, contours were refined with high- and low-speed diamond burs. After complete seating of the restoration, symmetry of shape (between teeth Nos. 7 and 10) was achieved. Interproximal embrasures, contacts, and prominent facial convexities/concavities (primary facial anatomy) were refined. Next, subtle depressions, constrictions, and angles (secondary facial anatomy) were developed. Finally, vertical and horizontal striations as well as roughness, dimpling, and minor incisal discrepancies (tertiary anatomy) were added. While intricate sounding, these post-milling adjustments took less than 5 minutes to achieve.
Based on the color mapping done previously, both restorations were stained, glazed, and then crystallized. Although advanced laboratory techniques, such as porcelain cutbacks, can be used to achieve custom anterior esthetics, effective use of the basic stains that come with a turnkey system such as the E4D Dentist are often all that is necessary to deliver impeccable results. In this case, four colors of stains were used to characterize the e.max crown on tooth No. 7. A basic dentin/cervical shade was used cervically and pulled to the mid-facial region. Incisal blue and grey were blended to various degrees and laid incisally and along the interproximal line angles. A dry brush was used to pull excess color and dampen these translucent areas as necessary. White stain was applied with an endodontic file and pulled vertically to create striations, hypocalifications, and an incisal halo.
After crystallization it was determined that the B1 block provided the most uniform color among adjacent teeth and would likely provide preferable esthetics over time. After the initial crystallization, the B1 e.max restoration still lacked the necessary amount of translucency along the incisal edge and mesial line angle. With the restoration seated in the mouth, a mixture of incisal blue and gray stain was applied with a paintbrush to mimic the appearance of the adjacent teeth. The restoration was carefully removed from the mouth and re-fired on the appropriate setting.
After the second firing cycle, the restoration was placed intraorally and the patient was delighted with the esthetics (Figure 8). In order to be absolutely certain of patient satisfaction, the restoration was cemented with clear temporary cement. The patient left with her permanent restoration provisionally cemented and was very pleased with the fit and esthetics. Two days later, the patient returned and the restoration on tooth No. 7 was removed and permanently re-cemented using Multilink Automix resin cement (Figure 9). The patient was then seen for a 1-week follow-up, during which she expressed her happiness over the esthetics and comfort of the permanently cemented restoration and surrounding gingival health.
On the day of the crown preparation and fabrication, the patient was in the dental chair for just over 3 hours. She was a cosmetically conscientious patient that did not look forward to the idea of wearing a provisional restoration that might not meet her esthetic demands. She was also aware that having a laboratory fabricate her restoration might require multiple try-in visits in order to achieve her desired result. Therefore, a longer single visit for same-day preparation and fabrication of the restoration was a much more acceptable option.
To maximize the potential of CAD/CAM systems, practitioners may find it necessary to step outside the boundaries of traditional dentistry and embrace skills and techniques normally reserved for laboratory technicians. By following an approach that merges efficient restorative techniques with concepts of visualizing color and texture, we can become better CAD/CAM dentists and offer impeccable, customized, same-day esthetics.
The author leads study clubs for D4D Technologies and has lectured on the E4D Dentist system, but has not received honoraria or other financial compensation from D4D Technologies for these activities.
Brent Harris, DMD
Private Practice
Port Saint Lucie, Florida


Figure 1 Figure 2 Figure 3

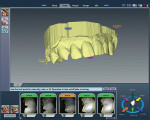
Figure 4 Figure 5 Figure 6

Figure 7 Figure 8