Newsletter
NewsletterJeff Files, DDS
This case involved a woman with occlusal dysfunction who was dissatisfied with her smile because of the unsightly display of gold crowns in her posterior and unattractive mottling on her anterior teeth. Factors such as a significant history of clenching and grinding, the management of active disease and infection, and the patient’s desire for an ideal or “media-generated” smile increased the difficulty of the case. As part of a comprehensive restorative plan that included disease control treatment, root canal therapy, and orthodontics to idealize tooth positioning, a Kois deprogrammer was used to evaluate the patient’s increasingly symptomatic, unacceptable function. In addition to reducing functional and biomechanical risks, the case resulted in improved esthetics with which the patient was highly pleased.
Often times patients seeking cosmetic improvements are unaware of other possible oral problems that may potentially be contributory to their esthetic issues. A thorough analysis of the patient’s oral condition can frequently lead to the realization that functional and biomechanical problems are prevalent. By performing a systematic assessment of not only the patient’s cosmetic condition but also the patient’s dental health risks and any active disease, a clinician can develop a comprehensive restorative treatment plan.
A 44-year-old woman presented for evaluation and improvement of her smile. Her chief complaint was the unattractive gold display of her posterior crowns coupled with unsightly “white spots” on her anterior teeth (Figure 1 and Figure 2). Her compelling purpose for seeking treatment was to achieve a “great smile.”
The patient’s medical history was noncontributory. In discussing her dental history, it was discovered that she had a significant amount of clenching and grinding, with reported nightguard use for more than 10 years. She experienced frequent morning headaches with or without the use of the nightguard. The patient also reported that tooth decay was a common finding at her dental examinations. She had previously been diagnosed and treated for periodontal disease but had inconsistent follow-up care. A comprehensive assessment was initiated to thoroughly evaluate her condition and provide predictable options for her care.
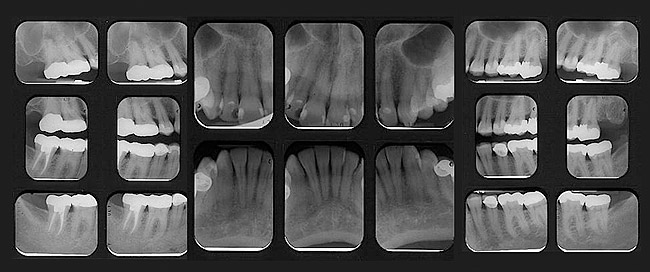
Periodontal: The periodontal evaluation revealed probing depths of 2 mm to 3 mm in the anterior sextants and 2 mm to 5 mm in the posterior sextants. Generalized light bleeding on probing was noted in the posterior. Radiographic examination revealed generalized mild to moderate horizontal bone loss of 1 mm to 3 mm. A vertical osseous defect was discovered on the mesial of tooth No. 15 with an associated probing depth of 5 mm (Figure 3). A periodontal diagnosis of AAP type II (mild periodontitis) was made.
Risk: Low
Prognosis: Good overall with a site-specific fair prognosis for tooth No. 15 due to the mesial vertical bony defect.
Biomechanical: The radiographic examination identified apical pathology on teeth Nos. 2 and 15 (Figure 3 and Figure 4). A diffuse, mixed radiographic lesion (Figure 4) was visible apical to teeth Nos. 3 and 4, having an appearance consistent with a mucous retention cyst.1 Clinically, teeth Nos. 2 and 15 both tested nonvital, while teeth Nos. 3 and 4 tested vital. Active tooth decay was found on teeth Nos. 15, 19, and 28. Teeth Nos. 2, 3, 12 through 15, 28, and 31 had defective, ill-fitting restorations. Teeth Nos. 2 through 4, 13 through 15, 18 through 20, and 29 through 31 were noted as structurally compromised due to the size, type, and depth of the restorations. Additionally, teeth Nos. 23 through 26 showed early signs of chemical erosion on the incisal edges. Tooth No. 3 presented with a bony exostosis on the buccal (Figure 5), creating short clinical crown height and a subsequent restorative compromise.
Risk: High
Prognosis: Poor with a hopeless prognosis for teeth with untreated tooth decay.
Functional: With most of the patient’s posterior teeth having been restored with crowns (Figure 6 and Figure 7) it was important to interpret the patient’s history and occlusal findings closely. The gold crowns on teeth Nos. 2 and 5 had holes worn in the occlusal surfaces with evidence of minimal wear on her other posterior crowns and natural dentition. Moderate wear was evident on the gold crown on tooth No. 31. A diagnosis of acceptable function could not be considered due to her long-term history of clenching and grinding, more than 10 years of nightguard use, joint sounds, and morning headaches. At the time of examination, she presented with tenderness to palpation of the right joint lateral pole rated at “5” on a scale of 1 to 10.2 Right masseter and temporalis muscles were also tender, with a rating of “5.” Load and resistance tests were normal. The right joint popped on opening with moderate intensity and had mild crepitus. There was no deviation on opening, and the range of motion was well within normal limits. Primary occlusal traumatism was noted on teeth Nos. 4 and 13. Teeth Nos. 6 through 11 and 22 through 27 were not touching in maximal intercuspation. Teeth Nos. 3 and 30 as well as Nos. 14 and 19 were in cross-bite (Figure 5 and Figure 8). The patient had an Angle’s Class I occlusion. A diagnosis of occlusal dysfunction was made given the history and examination findings.
Risk: Moderate
Prognosis: Fair
Dentofacial: Evaluation of the patient’s smile revealed medium maxillary lip dynamics and tissue display in a full smile (Figure 2). Uneven maxillary gingival levels, visible buccal bony exostosis on tooth No. 3, rotated and malposed teeth, mottling on multiple front teeth, a “reverse smile line,” tooth asymmetry, and an uneven maxillary occlusal plane were all significant findings in the dentofacial evaluation. The patient’s desire for an ideal or “media-generated” smile increased the case difficulty. The medium maxillary lip dynamics and subsequent tissue display created the risk evaluation for the case.
Risk: Moderate
Prognosis: Fair
The goal of treatment was to comprehensively address the patient’s dental health risks, active disease, and cosmetic desires. The first treatment goal was to manage active disease and infection. Following disease control therapy, comprehensive orthodontic therapy was recommended to idealize tooth positions to improve esthetics and function. After completion of orthodontic therapy, the author reassessed the patient’s esthetic desires and functional needs to create a comprehensive restorative plan.
Phase 1: Active Periodontal Therapy, Endodontic Therapy, Caries Control
Active periodontal therapy was performed to begin management of the patient’s early periodontal disease. Following active therapy, she was appointed for supportive periodontal therapy visits at 6-month intervals.
Root canal therapy was performed on nonvital teeth Nos. 2 and 15 (Figure 9). A composite restoration was placed in the endodontic access on the gold crown on tooth No. 2. Due to the presence of active caries, the gold crown on tooth No. 15 was replaced with a composite CAD/CAM-generated crown, which functioned as a long-term provisional restoration until orthodontic therapy was completed.3 A mesial-occlusal-distal (MOD) composite and a buccal composite were used to restore the carious lesions on teeth Nos. 28 and 19, respectively. Treatment was deferred on teeth with questionable restorations and structural compromises until completion of orthodontic therapy.
A caries management program was implemented consisting of in-office fluoride varnish applications at the patient’s re-care visits and daily at-home alkaline anti-caries rinses (CariFree® treatment and maintenance rinses, Oral BioTech, www.carifree.com).4 The high pH treatment rinse was used twice daily for 30 days, followed by ongoing use of the maintenance rinse twice daily.
Phase 2: Comprehensive Orthodontics
The patient was referred for a comprehensive orthodontic evaluation. The expectation of treatment was to level the maxillary occlusal plane, correct the rotations and cross-bites, and align the teeth, while improving tissue levels and function. The primary goal of orthodontics was to establish ideal tooth position for restorative treatment (Figure 10 through Figure 12).
Orthodontics was recommended for this patient to minimize the amount of tooth reduction that would have been necessary had her teeth remained malaligned. From a comprehensive treatment planning position, increased tooth reduction significantly weakens teeth, thereby increasing a patient’s biomechanical risk while reducing the long-term prognosis.5 An acceptable esthetic result is also less predictable when restoring malposed teeth.
Phase 3: Functional Management, Maxillary Restoration, Crown-Lengthening Surgery
The frequency and intensity of the patient’s headaches decreased significantly during orthodontic treatment. Several months following the completion of orthodontics, the patient again began complaining of muscle pain, headaches, and clenching and grinding symptoms with increasing frequency. Maxillary and mandibular alginate impressions were taken and casts were created for fabrication of a Kois deprogrammer.6 Resembling an orthodontic Hawley-type appliance, the Kois deprogrammer (Figure 13) consists of an acrylic lingual plate and a flat cingulum ramp that discludes all posterior teeth. The purpose of this appliance is to deprogram the muscles of mastication and permit the jaw to move to a neutral position in the joint space (a centric relation or adapted centric posture position). The deprogrammer is used to diagnose occlusal disease and evaluate patients’ symptoms as they relate to the temporomandibular joint (TMJ), functional concerns, clenching, and grinding. Patients are typically instructed to wear the appliance continuously (except while eating) and return in 2 to 3 weeks to confirm that they are “deprogrammed” (ie, confirm that the muscles of mastication are relaxed and the TMJs are in a consistent and reproducible position). Once confirmed, a bite record is taken for mounting patient models, functional planning, and treatment option development.
In this case, the Kois deprogrammer was used to evaluate the patient’s increasingly symptomatic unacceptable function. Her symptoms abated after wearing the deprogrammer for 2 weeks. An interocclusal recording of the “deprogrammed position” was made and study models were mounted in the adapted centric posture position on a semi-adjustable articulator for evaluation and treatment planning. Utilizing the mounting, premature and deflective contacts on the articulated models were adjusted, establishing an acceptable vertical dimension of occlusion7 at which the case would be treated. The interproximal extensions on the Kois deprogrammer were relieved, and the deprogrammer was placed on the master cast. The occlusal surface of the flat cingulum ramp was adjusted down to match the vertical dimension of occlusion established for the case. This procedure prepared the deprogrammer to provide a stable, repeatable occlusal guide for use at future clinical appointments.
Following the adjustment to the mounted master models, the models were sent to the laboratory for diagnostic waxing of teeth Nos. 3 through 14 to correct occlusion and improve esthetics in preparation for restorative care. It was requested that the laboratory wax to correct tissue levels on tooth No. 3, which had coronal tissue height and bony exostosis on the buccal, as well as tooth No. 12 where coronally positioned tissue created visual disharmony. The plan was to make the cosmetic corrections to the teeth and tissue and equilibrate the occlusion in concert with the restorative treatment. Using the diagnostic waxing, polyvinyl stents were fabricated for creating provisional restorations and to use as reduction guides during preparation.
The patient was appointed for preparation of teeth Nos. 3 through 14 as well as esthetic gingival correction surgery8-10 on teeth Nos. 3 and 12. Open-flap crown-lengthening surgery was performed on the buccal of tooth No. 3 by incorporating an internal bevel gingivectomy, elevating a full-thickness periodontal flap, and performing ostectomy and osteoplasty of the buccal bone and exostosis. The flap was then repositioned and sutured into place. A closed-flap esthetic crown-lengthening procedure was performed on the buccal of tooth No. 12. The procedure began with an internal bevel gingivectomy. The ostectomy was performed using a Wedelstaedt chisel intrasulcularly. Sutures were not required. Once the gingival contours were level and symmetrical, teeth Nos. 3 through 14 were prepared. Teeth Nos. 3, 4, 6 through 11, and 14 received composite core build-ups. Teeth Nos. 3, 13, and 14 were prepared for layered zirconia crowns, while teeth Nos. 4 through 12 were prepared for more conservative feldspathic porcelain restorations. Provisional restorations were fabricated using the polyvinyl stents created from the diagnostic wax-ups and a bis-acryl temporary material.
The patient was re-appointed 3 weeks later to evaluate tissue levels, confirm esthetic requirements, and manage the patient’s functional needs while in the provisional restorations.11,12 The Kois deprogrammer was lightly adjusted under the anterior ramp to assure a complete and passive fit around the provisional restorations on teeth Nos. 8 and 9. Undercuts were placed using a small high-speed round bur, and the deprogrammer was relined in the mouth using a firm, fast-setting bis-acryl material (Figure 13). The vertical dimension of occlusion was confirmed in the mouth and referenced on the master models. The deprogrammer was then used as an aid to guide the occlusal equilibration and fine-tune the occlusal scheme of the provisional restorations. Particular attention was paid to creating the correct anterior chewing envelope of function in the provisional restorations. Once the esthetics and function were correct, polyvinyl impressions of the provisional restorations were made and sent to the laboratory to communicate the exact shape and location of the final restorations. A face-bow record, interocclusal record (in the confirmed adapted centric posture position), and digital images were also captured for laboratory communication to be used in the creation of the final restorations.
Following seating of the restorations, the Kois deprogrammer was once again lightly adjusted on the anterior internal surface, relined in the mouth, and confirmed on the master models to manage the vertical dimension of occlusion. Occlusion of the definitive restorations was then fine-tuned using the relined Kois deprogrammer.
Phase 4: Mandibular Restorations
Mandibular restorations were completed using all-ceramic lithium-disilicate crowns on teeth Nos. 18 through 20, 29, and 30, as well as a composite restoration of tooth No. 21. The patient’s left side was treated first, followed by the right. When restoring each lower quadrant, the Kois deprogrammer was used as a stable repeatable point of reference to manage the occlusion. A maxillary nighttime splint was fabricated to protect the porcelain as a “belt and suspenders” approach to long-term management in an effort to do everything possible to decrease risk. The patient deferred treatment of teeth Nos. 2 and 31, which still have visible gold crowns, and No. 15, which is in a composite provisional crown.
The complexities of this case were identified, evaluated, and managed by utilizing the Kois Diagnostic Opinion Criteria (Kois Center, www.koiscenter.com). Once the functional, esthetic, and oral disease needs were identified, the Kois 10-Step Management System provided an effective means of managing and staging the treatment needed.
The Kois deprogrammer served as a convenient tool for diagnosis and predictable management of the presenting functional demands. It has been more than 1 year since the patient finished treatment. Her headaches have not returned and she reports that clenching and grinding have ceased. She is very happy with the final esthetics (Figure 14 through Figure 17) and the successful outcome of the case (Figure 9). Her overall prognosis is improved due to lowering the functional and biomechanical risks.
The author would like to thank: John C. Kois, DMD, MSD, and the Kois Center, Seattle, Washington; Dona Seely, DDS, MSD, of Dona M. Seely Orthodontics, Bellevue, Washington; and Leon Hermanides, ceramist and owner of Protea Dental Studio, Redmond, Washington.
1. Maestre-Ferrin L, Galán-Gil S, Carrillo-García C, Peñarrocha-Diago M. Radiographic findings in the maxillary sinus: Comparison of panoramic radiography with computed tomography. Int J Oral Maxillofac Implants. 2011;26(2):341-346.
2. Cont PC, de Azevedo LR, de Souza NV, Ferreira FV. Pain measurement in TMD patients: evaluation of precision and sensitivity of different scales. J Oral Rehabil. 2001;28(6):534-539.
3. Perry RD, Magnuson B. Provisional materials: Key componentsof interim fixed restorations. Compend Cont Educ Dent. 2012;33(1):59-62.
4. Young DA, Kutsch VK, Whitehouse J. A clinician’s guide to CAMBRA: a simple approach. Compend Contin Educ Dent. 2009;30(2):92-98.
5. Vailati F, Belser UC. Palatal and facial veneers to treat severe dental erosion: a case report following the three-step technique and the sandwich approach. Eur J Esthet Dent. 2011;6(3):268-278.
6. Jayne D. A deprogrammer for occlusal analysis and simplified accurate case mounting. J Cosmet Dent. 2006;21(4):96-102.
7. Adbuo J, Lyons K. Clinical considerations for increasing occlusal vertical dimension: a review. Aust Dent J. 2012;57(1):2-10.
8. Kois JC. Altering gingival levels: the restorative connection Part 1: biologic variables. Journal of Esthetic and Restorative Dentistry. 1994;6(1):3-7.
9. Kois JC. The restorative-periodontal interface: biological parameters. Periodontal 2000. 1996;11:29-38.
10. Bateman GJ, Karir N, Saha S. Principles of crown lengthening surgery. Dent Update. 2009;36(3):181-185.
11. Gratton DG, Aquilino SA. Interim restorations. Dent Clin North Am. 2004;48(2):487-497.
12. Bynum JH. Clinical case report: Testing occlusal management, previewing anterior esthetics, and staging rehabilitation with direct composite and Kois deprogrammer. Compend Contin Educ Dent. 2010;31(4):298-306.
Jeff Files, DDS
Private Practice
Redmond, Washington


Figure 1 Figure 2 Figure 4