Newsletter
NewsletterFuture technological developments that have the potential to change the industry
Over the last decade the dental industry has experienced a massive influx of new technologies. These advances have resulted in streamlined workflows as well as elevated product consistency and restorative accuracy, all of which have ultimately improved the level of patient care. For our 2013 Tech Issue, IDT presents three new developments that could potentially act as a catalyst for major changes in the dental arena. 3D printing, digital scanning material, and the process of growing bioteeth from stem cells represent major steps forward in science and technology, steps that are destined to move dentistry
ever further into the future.
3D Printing
GelSight Scanning Material
Bioteeth
How additive manufacturing stands to transform dental technology manufacturing processes
By Kate Hughes
Additive manufacturing, also known as 3D printing, is an emerging technology that has the potential to revolutionize product realization. As one of the fastest growing manufacturing technologies, it allows the layman to realize his own three-dimensional product designs without the need for a manufacturer—if he can dream it, he can create it. With nearly limitless potential applications, 3D printing encourages creativity and enterprise, giving anyone with vision the ability to hold that vision in his hands. Parents can create personalized toys for their children, bypassing the manufacturer and traditional retail store. Inventors can print prototypes and test new parts in a matter of hours and at a fraction of the cost, rather than waiting weeks to have them remotely manufactured at great expense. If the faucet in your bathtub breaks, perhaps one day you will be able to print a replacement. The possibilities are seemingly endless.
As one of 12 new technologies recognized by the McKinsey Global Institute as a “disruptive technology,” 3D printing has the potential to transform our lives, businesses, and the global economy (www.mckinsey.com). Already, this technology has left footprints in a number of diverse industries, with people printing everything from jewelry and food to clothes, guns, and medical devices. It is the latter application that has garnered the rapt attention of the dental laboratory industry with its potential for 3D printing end use products for clients. Only a handful of additive manufacturing companies are currently in the dental space, but those bringing the 3D printing movement to dental technology, are racing to develop new materials and applications that will expand 3D printing’s role in manufacturing dental devices and eventually be at the forefront of producing long-term end-use restorations.
3D printing technology is still an immature market. Only a small percentage of laboratories in the US are using 3D printing and laser sintering technology to efficiently deliver large numbers of structures in a single production cycle. According to Ron Snyder, head of business development at Envisiontec, Inc., the dental technology industry first began to pay attention to 3D printing when the technology matured to the level that copings and full contour crown and bridge wax patterns with intricate anatomical detail could be produced. “The anatomy displayed in these 3D printed wax patterns was far superior to anything we had previously been able to achieve,” says Snyder.
It wasn’t just the anatomical detail and time-savings that made 3D printing an attractive alternative to hand waxing. It was cost savings. Once the great potential inherent in additive technologies was realized, larger laboratories and manufacturers adopted the technology to reduce the cost of manufacturing precious metal restorations, especially in light of rising gold prices. Snyder explains, “In the past, when working on a precious metal full cast crown, a CDT would have to keep adding wax to create that high-end anatomical detail. By using 3D printing, laboratories were able to digitally optimize the thickness and consistency of the wax pattern through the CAD design software thus minimizing the amount of precious metal used in the casting process. In instances like this, switching from a manually produced full anatomical wax pattern to a 3D print-assisted wax pattern saved users a tremendous amount of money.”
From this starting point, additive manufacturing technology has mastered the production of more complex structures, such as partial denture wax patterns, implant surgical guides and working models as well as semi- and non-precious copings, titanium implant bars, long-term temporaries, and even denture bases. Today, 3D printing is generally accepted as an effective technology and offers a vast improvement over the time and resources required if a technician were to manually create these structures instead. This becomes truer as the technology continues to improve. “Now, 3D printing has the ability to deliver a lot of parts in a very short period of time, without putting financial strain on the laboratory. As a whole, 3D printing is a fast, cheap, effective solution that will almost certainly change the dental technology industry greatly in the years to come,” says Snyder.
Avi Cohen, Director of Global Dental for Stratasys, agrees that additive manufacturing technology has great potential but as with any new technology 3D printing is in need of a more mature market. However, as the technology matures and the market expands, the next huge frontier for additive manufacturing will be delivering products from the machine that will be directly placed in the mouth. “What I see is a movement, a very serious movement to the end-user approach,” says Cohen.
Research and development dollars are being spent on developing materials and more advanced technologies that can deliver an end product with the strength and durability to withstand the extreme environment and forces inherent in the human mouth. “There is a great deal of work going on right now,” says Patrick Dunne, Director of Industrial Applications Development at 3D Systems. “In terms of end product crowns, my feeling is initial developments will be through the photopolymer composite route.”
And that route would move forward from 3D printed temporaries to more sophisticated end products, says Robin Carden, Vice President of Research and Development at Glidewell. “We have an entire wing of our Research and Development center devoted to additive manufacturing technology and are experimenting with a number of
different materials.”
So how far away is research and development from delivering a 3D manufactured full-contour crown? The hurdle will be developing materials that are not only strong enough to withstand a harsh oral environment, but also esthetic enough to meet the high standards of today’s patients. It may be several years until that balance is achieved and a viable material reaches the market. However, Carden believes initial developmental breakthroughs will be realized in the next year or so. “New developments are coming very rapidly.” However, most of these experts believe that 3D printed zirconia will not be one of those new material developments. “When you try to mix zirconia powder with materials that would convert it to a flowable form along with binders to solidify the material, roughly only 50% of the material’s total volume is zirconia, not to mention the challenge of burning out those binders which results in a massive amount of shrinkage,” says Dunne. “Firing also never quite eliminates the porosity of the material and the carbon contamination caused by the binders trapped in the matrix destroy its mechanical properties.” However, Snyder says the ability to print materials such as zirconia is dependent on the type of 3D printing technology used. “We have been successfully testing the printability of zirconia for some time now,” says Synder. “Our unique ability to print highly viscous materials is an advantage. In our test laboratory porosity it not an issue and we’ve been able to achieve strengths that compare to some milled products.”
Even if an advanced ceramic or zirconia were developed, the challenge as Carden sees it is the ability of the technology to achieve acceptable translucency as well as the required high flexural strength and fracture toughness in the end product. He references a 2009 published study carried out at Aachen University in Germany where researchers, using a modified direct drop-on-demand inkjet printing unit, produced crowns from a zirconia-based ceramic suspension. “The problem with the resulting crowns was the lack of translucency and the ability to only achieve 763 MPa flexural strength,” explains Carden.
Dunne believes new material developments for producing a 3D machine-to-mouth end product such as a crown will begin with modifying photopolymer composite materials. “Advanced resin-based nano-ceramic structure material eliminates many of the problems associated with composites in the past,” says Dunne. “It doesn’t dull over time, is color stable, and is very tough. Although, as with any new product, there are still unknowns in respect to long term durability.” Techniques are evolving he says that are capable of 3D print processing composite materials that have been altered into a toothpaste-type viscosity.
Carden agrees that composite materials such as 3M ESPE’s Lava™ Ultimate will be the starting point but takes the vision a step further by envisioning the creation of a hybrid crown composed of a polymer composite base deposited by one printing nozzle and a 50/50 mixture of a nano zirconia polymer deposited by a second printing nozzle to add strength to the end product. And if a multiple nozzle technology were developed, it opens the door to printing multiple shades over the base material. “Imagine a main printing nozzle with multiple nozzle arms like an octopus coming down around it,” says Carden. “Each of the arms would be controlled by a computer-controlled gate system to deposit patient-specific shades to the restoration.”
Eventually Carden says advanced 3D technologies will allow the manufacture of end product crowns using advanced lithium silicate or disilicate materials, but new printing technology with very high temperature nozzles to melt the glass ceramic as it moves out of the nozzle will need to be developed.
“We must consider that printing glass/ceramic composite materials strong enough for permanent restorations requires a lot of heat,” explains Carden. “The machines currently on the market are not equipped to handle those temperatures. Creating technology that can print those materials is something that can definitely happen down the line.”
Closer to developmental reality are materials and applications for additive manufacturing that would allow production of flexible partials with the biocompatibility and strength to be placed directly in the patient’s mouth, orthodontic aligners thermo-formed over a series of 3D printed models that are CAD designed to project corrective tooth realignment over a period of time, or even dentures complete with teeth and characterized with a variety of colors. “The biggest challenge at the moment is developing materials that are biocompatible and strong enough to withstand the extreme conditions of the oral environment,” says Cohen. “In terms of mechanical properties, the materials would need to perform the same on day one in the mouth as day 1000.” And if such materials were to be developed, it would open the door for other end products such as anti-snoring and bruxism devices.
While its many applications are currently in the research and developmental phases, 3D printing has the potential to cause major disruptions in the dental technology industry. Many of these changes are positive. 3D printing allows laboratories to make inexpensive prototypes in a relatively short period of time or reverse engineer large complex cases for patient try-in prior to committing to final case completion. In addition, because 3D printing creates objects via additive manufacturing, rather than cutting material away in subtractive processes, it wastes less material, leading to cost savings.
3D printing also allows dental laboratories to maximize productivity while minimizing labor, as so much of the process is automated. Dunne says that in terms of sheer volume and labor hours, there is no comparison between hand-made restorations verses restorations made with a machine. Automated systems will always have a higher output and require less labor. “The new technologies available in dental technology, especially 3D printing, allow laboratories to dramatically increase their output while maintaining or even reducing their units of labor,” he explains. And because these 3D printers can work 24 hours a day, 7 days a week, laboratories can now meet a much higher demand.
3D printing is a rapidly emerging technology that has the future potential to change the manufacturing structure of the dental laboratory industry. Although the technology is still in its infancy, rapid advances in new materials and 3D printing equipment are on the not so distant horizon. As with any new technology, the barriers to entry are cost and speed of production. But all that could change and change quickly as the practicalities of the technology better and more fully meet the needs of the end user. After all, a decade ago, few businesses in this industry owned a scanner and the only product being produced by automated manufacturing was a zirconia substructure.
Just last year, Dr. Jules Poukens, a cranio-maxillofacial surgeon and professor at the University of Hasselt in Belgium performed a full jaw replacement using a 3D printed mandible made from titanium by Layerwise, a metal-focused additive manufacturer, and infused the jaw with a bioceramic coating compatible with the patient’s tissue. Today, Poukens’ team is working on methods of 3D printing artificial bone infused with patients’ own stem cells, to create a material that not only restores function, but also hastens the patient’s healing process.
Poukens says that the reason their material was developed to work in tandem with 3D printing technology is because it allows them to customize every reconstructive prosthetic to each individual patient. “Giving patients a custom fit prosthesis is the best possible way to ensure a procedure’s success,” he says.
Researchers are not just concerned with 3D printing’s applications in dental technology, but in medicine in general. Biomedical applications for 3D printing are being discovered every day, with companies 3D printing pills, futuristic casts, and even functioning human organs. One such researcher is Michael McAlpine, an assistant professor of Mechanical and Aerospace Engineering at Princeton University. Recently, McAlpine’s research developed, and 3D printed, a bionic ear. Not only could this ear ultimately allow deaf people to hear (similar to a cochlear implant), but it could also give people with normal hearing the ability to hear frequencies normally unrecognizable by a normal human ear. According to McAlpine, 3D printing was the best method for creating this bionic organ, as it allowed them to ‘grow’ both the ear and the electronics together, at the same time. “We turned to 3D printing because the technology allows you to go layer-by-layer, which means that the electronics and living tissue can be intertwined. It’s just a new avenue that we can use to achieve our research goals in bioelectronics,” says McAlpine.
As a “disruptive” technology, 3D printing has the capability to drastically change the way many industries do business. Also, because it is so open-ended, many companies have used 3D printing for novelty purposes. However, the novelty 3D printing endeavors may have far-reaching effects on the dental technology industry without ever even intending to. Take for example “Clone Factory,” a Japanese company that, for the price of about $1,300, will scan a person’s face and have their features 3D-printed onto an 11-inch doll. While this is a really interesting niche market, the ability to 3D print human faces with photo-realistic accuracy could be extremely useful in the medical field. Imagine if technicians were able to 3D print a patient’s entire head, including the inside of their mouth, with 100% accuracy. From there, they could conduct try-ins and modify restorations to achieve functional and esthetic perfection, even if they never get the opportunity to meet the patient in person. They could treat patients on the other side of the planet just as effectively as they would be able to treat a patient who lives right next door.
New technology captures highly detailed images for 3D reconstruction
By Pam Johnson
Scientific breakthroughs don’t always happen while researchers are peering through microscopes or monitoring brain activity in real-time. Sometimes that spark of invention or inspiration comes from watching the simplest of human activity—like a baby exploring the world through its sense of touch.
That is exactly how it happened for Edward Adelson, professor of Vision Science at MIT’s Department of Brain and Cognitive Sciences. He was fascinated watching his two young children explore their new world by touching everything they came in contact with, and even as infants perceive detailed information about each of those objects. He knew how very sensitive tactile perception could be and that human skin can sense the surface topography of an object down to the submicron level. Each time we touch something or something touches us, the skin on our bodies distorts to the shape and form of that object. We can sense the heat or coldness of the object, the shape or bulk, or the dryness and wetness as thousands of receptors spring into action and transmit the sensed information to our brains.
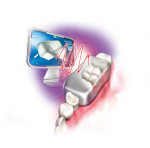
As a researcher involved heavily in the neurosciences, Adelson wondered if a sensor could be developed that would react much in the same way as our skin and convert that sense of touch into an image. It was this inspiration that led him on the path to invent GelSight (www.gelsight.com), a material with specialized illumination and imaging that can record and digitize anything it comes into contact with. “The concept behind GelSight is a clear, elastomeric material covered with an opaque reflective skin or coating,” says János Rohály, a high-tech entrepreneur who was co-founder of Brontes Technologies, the company responsible for the development the 3M ESPE Lava™ C.O.S. digital impression device and is now one of the co-founders of GelSight. “The reflective coating deforms much like human skin does when it comes into contact with an object and captures data about its shape and topography. A camera behind the clear gel captures images from the sensor and digitizes them.” As the gel’s reflective membrane deforms, multiple light sources illuminate the deformation from different angles and a single camera captures the highly detailed image for three-dimensional reconstruction of the measured surface.
GelSight is a platform technology, meaning it is universally applicable in many fields irrespective of the object, the material, or the particular measurement context. Already, the company has designed and manufactured prototypes of the technology for clients involved in different industries, such as the solar industry and the paint industry. The solar industry uses GelSight to detect the microtextured surface features of self-cleaning glass, whereas the paint industry uses it to develop microtextured coatings with unique surface characteristics that enable large cargo ships to decrease fuel consumption by 2%, providing the industry with $8 billion dollars in savings per year. GelSight is also being used to measure the functional surface topography of medical or dental implants where surface roughness is critical.
One of the unique features of this material is that it is agnostic to the optical properties of the material it comes in contact with. “We basically solved the problems of capturing 3D shapes of any material, regardless of the optical properties of the object we are scanning,” says Rohály. Having been involved in the development of the Brontes digital intraoral scanning technology, he understands the limitations of the current technologies being used in dentistry to capture tooth morphology, shape, and form in the oral environment. “GelSight captures hard and soft tissue regardless whether it is wet, dry, translucent, or shiny,” he explains.
Although Rohály admits that the company is currently not pursuing applications in dentistry for this technology, he does believe it could be incorporated as a hybrid technology to capture digital data in the oral environment. Used in somewhat the same fashion as traditional impression material, it would come in contact with the surface of the teeth, but unlike traditional impression material, the gel would instantaneously capture topographical data of the complete tooth surface and digitally transmit that data to a computer screen. “It is certainly feasible to think about the gel functioning in a similar way as traditional impression material. The difference would be that GelSight could capture the surface morphology instantaneously, eliminating the need for patients to endure several minutes of curing time,” says Rohály. “We actually mounted one of these GelSight plates on an intraoral camera to demonstrate its ability to capture surface detail.”
But intraoral capture of tooth preparations is not the only application Rohály believes GelSight could have in the field of dentistry. The ability to capture data at the submicron level might also be used to detect and measure changes over time in the patient’s oral condition. “The ability to capture a single arch or the ability to measure submicron areas to measure change with single micron reliability might also prove useful in detecting the effects of bruxism for example or periodontal loss,” says Rohály. “There is no digital intraoral technology currently on the market that has that level of resolution capability.”
The Dollar’s Details
For a video showing the level of detail GelSight is capable of capturing, please visit the link below. dentalaegis.com/go/idt398
New research takes growing bioengineered teeth one step closer to reality
By Pam Johnson
The next generation of practitioners may one day have a clinically viable system for using harvested cells from their patients’ mouths to grow a replacement tooth for an edentulous site or to use as a repair material for diseased teeth. The quest to find a practical cell-based method for replacing a missing tooth with a natural biotooth continues to be the holiest of dental research grails and may be a step closer to reality, based on the results of research being conducted by Professor Paul Sharpe and his team at King’s College London.
In the past dental research teams have focused on using cells from embryonic tissue, “programming” the cells to form a primordial tooth form, and then transplanting that primordial tooth in an animal’s mouth where it would grow into a natural tooth.
“Growing teeth outside the host body has been fairly easy,” says Sharpe. “However, when transplanted these bioengineered teeth are still missing some essential elements such as the complete root and periodontal tissues. And, for any kind of viable and practical dental therapy, we will not be able to use embryonic cells to induce the tooth growing process.” Teeth form from two types of cell populations: epithelium cells and mesenchyme cells. Mesenchyme, or stem cells, are immature non-specialized cells that can differentiate into multiple specialized tissue cell types such as heart muscle, nerves, or bone. Most often stem cells are associated with embryonic tissues, however advances in research have found that viable adult stem cell populations can be found in bone marrow and even exfoliated baby teeth. However, these types of adult stem cells still need to be stimulated by embryonic tissues in order to reproduce and grow. And because sources for embryonic stem cells are limited, Sharpe set out to find a more readily accessible source of adult human stem cells that could be manipulated and induced to act in much the same way as an “unprogrammed” embryonic cell.
“In 2004 we showed that you can take adult stem cells from bone marrow and combine them with embryonic tooth epithelium from a mouse and grow a viable mouse tooth in situ,” explains Sharpe. Although this was a ground-breaking discovery in this field of research, locating a source of adult stem cells without need for medical surgery was again an issue, particularly when thinking in terms of the dental practice and the practicalities of harvesting cells that possess the tooth-growing properties needed to reproduce all the essential structures of a natural tooth.
For the past decade Sharpe has been on a quest to find a systematic approach that could be carried out in a dental setting and yield an unlimited supply of cells from an adult patient. What he discovered is that when epithelial cells culled from the gingiva of adult patients are used in combination with mouse embryonic mesenchyme cells, a viable and complete tooth system can be created. Now, at least, an unlimited source of human oral epithelial cells that can be induced to grow a natural human tooth has been identified. However, the challenge for ongoing research is to discover a viable laboratory process that can produce or stimulate the embryonic properties in adult stem cells that is needed to induce tooth formation. “If you combine the epithelial cells from gum tissue with mesenchyme cells from human bone marrow, you will never be able to grow a tooth,” says Sharpe. “The adult bone marrow stem cells do not possess the embryonic properties that will induce the tooth growing process.” Sharpe has shown, however, that when the epithelial human gingival tissue is combined with human embryonic tooth stem cells this combination will result in the growth of a human tooth. So now the search is on in the laboratory to eliminate the need for embryonic stem cells and find a way to make adult stem cells behave like embryonic tooth stem cells. When this is accomplished, then a cost-effective process for harvesting oral tissues for the growth of human teeth in the dental setting can be developed to offer patients a viable alternative to traditional implant restorative treatment.
The human tooth culturing process, transplant, and growth procedure would take about nine to 10 months to complete, Sharpe speculates. The patient would come into the dental office for the harvesting process whereby the clinician would remove a small amount of healthy epithelial gum tissue. The tissue would be sent to a laboratory where the cells would be combined with mesenchyme cells and induced to grow over a four to six-week period into a primordial tooth form. The primordial biotooth “seed” would then be sent back to the dental clinic and placed in the edentulous site to mature, develop, and grow into a fully functional tooth over a five- to six- month period.
Sharpe admits that dental research is a long way away from being able to transplant a biotooth in a human, but believes that with such therapies near on the horizon, dental schools around the world should begin to develop educational courses that teach about the latest research being carried out in research laboratories. To that end, a new one-year master’s course at Kings College in London will be offered this September for graduate students to learn and get hands-on experience on how to grow tooth cells and create these bioteeth. “There also needs to be an increasing shift in the next 10 to 15 years toward teaching under graduates about the types of research being conducted in the dental field,” Sharpe concludes.