 Newsletter
NewsletterCase reports describe two children, each with two double primary incisors.
By Theodore P. Croll, DDS | Constance M. Killian, DMD
Defining the exact essence of a dental twinning phenomenon can be a difficult or impossible diagnostic task. Tooth twinning, also called doubling or schizodontia, represents certain kinds of tooth malformations with orthodontic, restorative dentistry, and appearance implications. The three chief types of dental twinning have traditionally been called gemination, fusion, and concresence.1,2 Gemination is thought to be when one enlarged tooth appears as if the clinical crown has two portions; that is, the crown of one tooth has twinned. If two coronal portions are not evident, the larger tooth is sometimes referred to as a macrodont. A geminated anterior tooth has one root, which is often wider than a normal root. Fusion is defined as two teeth that physiologically combine to varying degrees during the early odontogenic course; generally, two discernable roots and root canal systems are seen radiographically. Concresence is when two teeth are joined by cementum. Diagnostic uncertainty can result when the degree of fusion of the teeth, the presence of a supernumerary tooth, or the congenital absence of one or more teeth are considered.3
This report documents two cases in which children have two double teeth in the primary dentition and reviews clinical and radiographic findings in search of diagnoses.
A 5-year, 5-month-old male patient presented for a routine examination. The only remarkable findings were a discolored maxillary right primary central incisor, which had suffered previous trauma, and the two mandibular primary lateral incisors were double (Figure 1). Vertical grooves—labial and lingual—demarcated two distinct coronal segments in each double tooth. A radiograph of the region showed that each of the doubled teeth had two discernible roots and root canals (Figure 2). In each tooth, the most distal coronal segments appeared to resemble a normal primary lateral incisor shape. The mesial coronal portions appeared somewhat conical in shape, similar to a microdont that dentists routinely call “a pegged lateral incisor.” The underlying permanent central incisors and succedaneous lateral incisors appeared to be normal. There was no evidence of missing, extra, or double permanent anterior teeth.
When all of the clinical and radiographic information was summarized, the authors concluded that the normal primary lateral incisors had fused during their development with supernumerary primary lateral incisors, which had formed on the mesial aspects of the normal teeth.
A 4-year, 9-month-old male Caucasian was examined at a routine preventive dentistry recall appointment. He had a double tooth in both the maxillary and mandibular right primary lateral incisor regions (Figure 3). Both twinned teeth had labial and lingual vertical grooves running the full coronal length of the crowns. The maxillary twinned tooth showed two distinct roots and canal systems on the radiograph (Figure 4). The lingual groove was carious, and resin-modified glass-ionomer restorative cement was used for restoration. There were no extra or missing permanent incisors seen on the film. The authors surmised that the maxillary right primary lateral incisor had fused with a supernumerary incisor during their formation.
The mandibular double tooth posed a more difficult diagnostic challenge. While the crown section appeared as wide as two normal teeth (Figure 3), there was only one root and one root canal system evident on the radiograph (Figure 5). No extra permanent incisors were seen radiographically, and none were missing. Because both right permanent incisors were present on the radiograph, a dental anlage from a primary tooth would have been necessary for development of each permanent incisor. Therefore, the authors concluded that the mandibular primary right lateral incisor had.complete radicular fusion with the neighboring primary central incisor, along with coronal fusion.
The case encountered by the authors that most clearly demonstrates the concepts of tooth fusion and gemination involved a 5-year-old male with both defects in his maxillary primary incisors. The authors surmised that the boy had a geminated primary maxillary right central incisor, and that the primary left central incisor was fused with the primary left lateral.2,3
Duncan and Helpin published a case report of bilateral fusion involving mandibular primary central and lateral incisors. Their report offered a literature review regarding “bilateral occurrence of fusion and gemination in the primary and permanent dentitions.”4 As part of their review, they considered 11 literature articles that reported the prevalence of double teeth and bilateral double teeth in the primary dentition. The sample sizes of patients evaluated in those 11 research reports ranged between several hundred and 8,500. Duncan and Helpin summarized all the patients evaluated in those reports and came up with 23,986 people. Among them, double teeth were seen in 115 (prevalence of 0.5%), and bilateral double teeth were seen in only five patients (prevalence of .02%).
Schurs and van Loveren published an extensive review of the subject of “double teeth,” citing 273 literature references on the subject. Their article expounded on nomenclature, diagnostic criteria for fusion and gemination, morphology and anatomy, jaw location, gender, prevalence, bilateral double teeth, triple and quadruple teeth, and pathogenesis of such anomales.5 In their introduction, they maintain, “The etiology and pathogenesis of double teeth is still enigmatic, and even their frequency is uncertain.” Although much uncertainty exists about the nature of dental duplication, there are some findings that can be gleaned from the Schurs/van Loveren review, including the following:
However, the exact nature of such anomalies remains unresolved. In 1990,3 the authors r.commended that when diagnosing the clinical condition of combined or enlarged teeth, the general terms dental twinning, doubling, or even triplication6,7 be used, rather than ascribing precise terms such as gemination, fusion, or macrodontia. The term duplication can also be used when referring to such anomalies. Academic conjecture as to the actual developmental nature of any one anomaly can be made for descriptive purposes, but when the definitive biologic essence of a defect cannot be proven, only a diagnostic supposition can be made, as was done in these two cases. In Case 2, the diagnostic analysis would have been much different had the mandibular permanent right lateral incisor not been present radiographically. In that case, it could be conjectured that the primary central incisor was geminated and the primary lateral incisor was congenitally absent. Likewise, it might have been suggested that the mandibular primary lateral incisor was absent and the primary central incisor had fused.completely with a supernumerary incisor. Even though there was only root in the mandibular double tooth in Case 2, we could not call the doubling gemination. There could not have been a permanent successor to the primary lateral incisor without an embryological predecessor. The only logical explanation would therefore be.complete radicular fusion of the primary lateral and central incisors. Such speculating shows how difficult it can be to make assured assessment of the developmental events causing dental doubling or tripling, and highlights the need to evaluate all clinical and radiographic findings to analyze any one case.
1. Levitas TC. Gemination, fusion, twinning, and concresence. ASDC J Dent Child. 1965;32:93-100.
2. Croll TP, Rains NJ, Chen E. Fusion and gemination in one dental arch: report of case. ASDC J Dent Child. 1981;48(4):297-299.
3. Killian CM, Croll TP. Dental twinning anomalies: the nomenclature enigma. Quintessence Int. 1990;21(7):571-576.
4. Duncan WK, Helpin ML. Bilateral fusion and gemination: a literature analysis and case report. Oral Surg Oral Med Oral Pathol. 1987;64(1):82-87.
5. Schuurs AH, van Loveren C. Double teeth: review of the literature. ASDC J Dent Child. 2000;67(5):313-325.
6. Prabhakar AR, Marwah N, Raju OS: Triple teeth: case report of an unusual fusion of three teeth. ASDC J Dent Child. 2004;71(3):206-208.
7. Schulz-Weidner N, Ansari F, Mueller-Lessmann V, Wetzel WE. Bilateral triplicated primary central incisors: clinical course and therapy. Quintessence Int. 2007;38(5):395-399.
Theodore P. Croll, DDS
Private Practice
Doylestown, Pennsylvania
Affiliate Professor
Department of Pediatric Dentistry
University of Washington School of Dentistry
Seattle, Washington
Adjunct Professor
University of Texas Health Science Center at San Antonio Dental School
San Antonio, Texas
Constance M. Killian, DMD
Private Practice
Doylestown, Pennsylvania
Adjunct Associate Professor of Pediatric Dentistry
University of Pennsylvania
Philadelphia, Pennsylvania
To read another article by Dr. Croll, visit: dentalaegis.com/go/id93

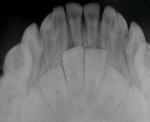
Figure 1 Figure 2 Figure 3

Figure 4 Figure 5














