Newsletter
NewsletterAn interdisciplinary team approach to esthetic implant treatment planning is key to a successful esthetic outcome.
By Robert Levine, DDS | William Martin, DMD, MS
The addition of dental implants as a viable and predictable treatment option has had life-changing benefits for many patients. The improvements psychologically, medically, and socially are the results of clinicians’ ability to replace missing teeth with permanent root substitutes, avoiding conventional fixed or removable restorations. The interdisciplinary team approach to patient care is especially important when the treatment involves the esthetic zone. The implant reconstruction requires comprehensive preoperative diagnosis and planning, followed by precise surgical and restorative procedures that maximize implant positioning and restoration to mimic the missing dental unit(s).1-3
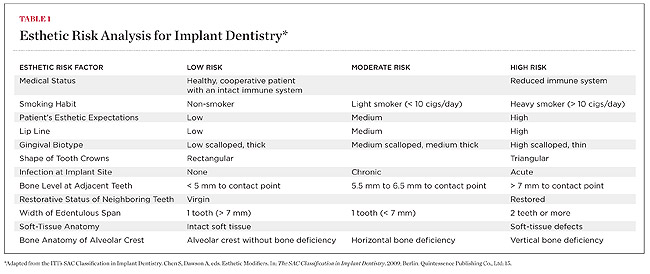
Treatment with dental implants in the anterior maxilla is an advanced or complex procedure based on the International Team for Implantology’s (ITI) Straightforward, Advanced, Complex (SAC) Classification of Implant Dentistry.4 The SAC Classification System has both restorative and surgical categories that use a normative classification system, which can be influenced by modifying factors based on individual clinical situations. One area that can influence this classification—both from a surgical and restorative perspective—is found in the ITI’s “Esthetic Risk Assessment (ERA) analysis” (Table 1).5
ERA is a pretreatment assessment tool that uses clinical precursors to determine the risk of achieving an esthetic result based on known surgical and restorative approaches in given clinical situations. Esthetic risk factors should be addressed directly with the patient before the initiation of treatment to avoid any posttreatment misunderstandings that may result from unmet high expectations. The clinician can best avoid potential posttreatment complications and an unhappy patient by gathering information chairside with patients during their consultation visit and sharing it with them using aids such as the ERA form.2,4,5 This is an excellent communication tool that can be used in all esthetic cases to help both the clinician and the patient achieve their esthetic goals. The more high-risk categories the patient falls into, the more conservative the surgical and restorative approach should be.6 This will help avoid any potential esthetic disasters later.
The following case examples highlight the use of the ERA in treatment planning patients who want to replace failing and missing teeth in the esthetic zone.
A 22-year-old healthy woman re-presented nearly halfway through 2 years of full-banded orthodontic therapy to correct a 4-mm midline discrepancy (to the patient’s left side), with the result being a space too small for implant placement in site No. 10 and a space too large in site No. 7 (Figure 1). Included as part of the team’s treatment of orthodontic patients in preparation for dental implants were periodic office visits to the periodontist/implant surgeon’s office to re-evaluate the inter-root spaces and need for additional space adjustments based on periapical radiographs and clinical assessments for proper implant placement. A cone-beam computed tomography (CBCT) scan was taken of the maxillary jaw to evaluate bone availability for both implant sites at an initial visit to help in determining the sequencing of surgical treatment. While a large horizontal-ridge defect requiring bone reconstruction was noted for site No. 7, adequate ridge width for a 3.3-mm width implant was noted for site No. 10. The authors’ surgical and prosthetic goals were to place 12-mm x 3.3-mm narrow-connection bone-level implants (Straumann®, www.straumann.us).7
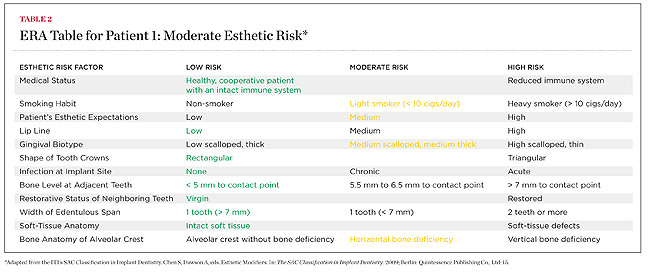
A tentative team treatment plan was reviewed with the patient from the outset of orthodontic therapy, so she was educated as to what the overall time and surgical/prosthetic treatment costs would be once orthodontics was completed. Evaluation of the patient’s esthetic risk factors was reviewed with her (Table 2) at the CBCT visit, and the following restorative-driven treatment plan was developed, discussed, and finalized with her orthodontist and restorative dentist, and included the following steps.
A male patient presented for an implant consultation with missing teeth Nos. 8 through 10, which he reported had been fractured at the “gum line” 4 months earlier as a result of an accident (Figure 6 and Figure 7). He also reported that the roots of the teeth had been extracted and grafts placed by his dentist in his hometown soon thereafter. A clinical and radiographic examination (with a radiographic template) was performed to allow the implant team to discuss the available treatment options. The panoramic radiograph revealed retained root tips in site Nos. 8 to 10 (with periapical radiolucencies), which appeared to be covered by a grafting material (Figure 8). The patient was informed that the root tips needed to be removed along with the graft material prior to the initiation of definitive implant therapy. During the treatment planning discussions, the patient informed the authors of his desire for individual fixed implant-supported restorations. He was educated on the pros and cons of this approach with regard to implants in site Nos. 9 and 10, which could negatively affect the inter-implant crest height, papilla, and esthetic outcome.9-12 He elected to have implants placed in the central sites and have a cantilevered restoration in site No. 10. Placing implants in sites Nos. 8 and 9 would help maintain the symmetry of the restorations while maximizing available tissue from the nasopalatine area for papilla formation.
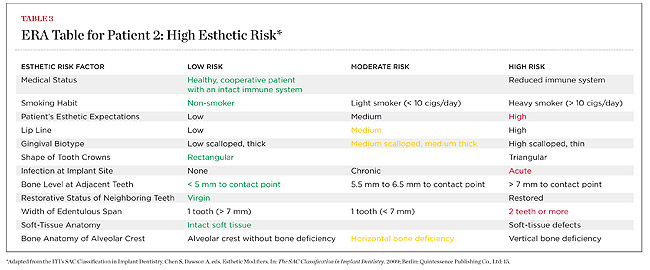
During the pretreatment process, an ERA analysis revealed a high risk of failure to achieve an ideal esthetic result (Table 3). Clinical factors that greatly influenced this rating were:
• High esthetic demands.
• Acute infection of the remaining roots in site Nos. 8 through 10.
• An extended edentulous area coupled with a horizontal-ridge deficiency.
The patient was made aware of the esthetic risk and elected to proceed with the following treatment plan:
The comprehensive treatment of implant therapies using the team approach concept works to benefit patients. As the medical model has shown, members’ knowledge of their respective areas contributes to the overall success of the rehabilitation, which becomes even more important in cases involving the esthetic zone.2,3,17 The routine use of the ERA analysis helps in careful surgical and restorative interdisciplinary diagnosis and planning. This results in a functional and esthetic outcome as well as a satisfied patient.
The authors would like to thank the following treatment teams: For Patient 1, periodontist Robert A. Levine, DDS, Philadelphia, Pennsylvania; restorative dentist Harry Randel, DMD, Philadelphia, Pennsylvania; orthodontist Harold Middleberg, DMD, Philadelphia, Pennsylvania; and laboratory technician Felix Levitsky, CDT, Ceramic Art Dental Studio, Huntingdon Valley, Pennsylvania. For Patient 2, oral surgeon Emma Lewis, BDS, MBBS, Gainesville, Florida; restorative dentist Will Martin, DMD, MS, Gainesville, Florida; and laboratory technician Mitchell Jim, CDT, of Gainesville, Florida.
1. Cordaro L. Implants for restoration of single tooth spaces in areas of high esthetic risk. In: Dawson A, Chen S, Buser D et al, eds. The SAC Classification in Implant Dentistry. Quintessence Publishing; 2009:50-56.
2. Levine RA, Nack G. Team treatment planning for the replacement of esthetic zone teeth with dental implants. Compend Cont Ed Dent. 2011;32(4)44-50.
3. Levine RA. Guest editorial. Functional Esthetics and Restorative Dentistry. 2008;2(3):2.
4. Buser D, Martin W, Belser UC. Optimizing esthetics for implant restoration in the anterior maxilla: anatomic and surgical considerations. Int J Oral Maxillofac Implants. 2004;19(Suppl):43-61.
5. Martin W, Morton C, Buser D. Pre-operative analysis and prosthetic treatment planning in esthetic implant dentistry. In: Buser D, Belser U, Wismeijer D, eds. ITI Treatment Guide I: Implant Therapy in the Esthetic Zone: Single Tooth Replacements. New Malden, Surrey, UK: Publishing Co Ltd; 2007;1:9-24.
6. Buser D, Halbritter S, Hart C, et al. Early implant placement with simultaneous guided bone regeneration following single-tooth extraction in the esthetic zone: 12-month results of a prospective study with 20 consecutive patients. J Periodontol. 2009;80(1):152-162.
7. Atieh MA, Ibrahim HM, Atieh AH. Platform switching for marginal bone preservation around dental implants: a systematic review and meta-analysis. J Periodontol. 2010;81(10):1350-1366.
8. Levine RA. Implant site preparation: Horizontal ridge augmentation using particulate allograft and the principles of guided bone regeneration. In: Sonick M, Hwang D, eds. Implant Site Development. Hoboken, NJ: Wiley-Blackwell, 2012:179-201.
9. Tarnow DP, Cho SC, Wallace SS. The effect of inter-implant distance on the height of inter-implant bone crest. J Periodontol. 2000;71(4):546-549.
10. Cardaropoli G, Wennstrom JL, Lekholm U. Peri-implant bone alterations in relation to inter-unit distances. A 3-year retrospective study. Clin Oral Implants Res. 2003;14(4):430-436.
11. Tarnow D, Elian N, Fletcher P, et al. Vertical distance from the crest of bone to the height of the interproximal papilla between adjacent implants. J Periodontol. 2003;74(12):1785-1788.
12. Gastaldo JF, Cury PR, Sendyk WR. Effect of the vertical and horizontal distances between adjacent implants and between a tooth and an implant on the incidence of interproximal papilla. J Periodontol. 2004;75(9):1242-1246.
13. Hinds KF. Custom impression coping for an exact registration of the healed tissue in the esthetic implant restoration. Int J Periodontics Restorative Dent. 1997;17(6):584-591.
14. Linkevicius T, Vindasiute E, Puisys A, Peciuliene V. The influence of margin location on the amount of undetected cement excess after delivery of cement-retained implant restorations. Clin Oral Implants Res. 2011;22(12):1379-1384.
15. Wadhwani C, Pineryo A. Technique for controlling the cement for an implant crown. J Prosthet Dent. 2009;102(1):57-58.
16. Wilson TG Jr. The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. J Periodontol. 2009;80(9):1388-1392.
17. Present S, Levine RA. Single maxillary anterior tooth restoration. Case to replace a non-restorable maxillary left canine illustrates a team approach. Inside Dentistry. 2010;6(1):58-66.
Robert Levine, DDS
Private Practice at the Pennsylvania Center for Dental Implants & Periodontics
Philadelphia, Pennsylvania
Clinical Professor of Periodontology and Implantology
Kornberg School of Dentistry at Temple University
Philadelphia, Pennsylvania
William Martin, DMD, MS
Associate Professor and Director of the Center for Implant Dentistry
University of Florida, College of Dentistry
Gainesville, Florida
Table 1
Table 2
Table 3


Figure 1 Figure 2 Figure 3

Figure 4 Figure 5 Figure 6


Figure 7 Figure 8 Figure 9


Figure 10 Figure 11 Figure 12