Newsletter
NewsletterAdvanced digital tools help improve accuracy, predictability
By Jeffrey Ganeles, DMD | George A. Mandelaris, DDS, MS | Alan L. Rosenfeld, DDS
Surgical guides are created by combining diagnostic anatomical information from a computerized tomography scan with physical or virtual representations of the planned restorations. Today, most diagnostic scans are accomplished using cone-beam computed tomography (CBCT) scanners. Office- or laboratory-fabricated radiopaque scanning appliances may be used to simulate the desired position of teeth, midline access holes, tissue deficits, etc.1 These dental restorative landmarks must be analyzed and compared to the patient’s underlying radiographic anatomy, enabling decisions about implant position, size, grafting requirements, and other parameters. When this computer-based planning technology is used to create surgical guides, the process becomes known as “computer-assisted manufacture surgical guidance.”2
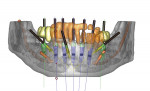
Digital data provide the foundation for creating models, surgical guides, and restorations from the same information. For this analysis, medical modeling of the data can be performed, converting it to 3-dimensional (3D) virtual images. Rapid prototyping3 and 3D printing, or stereolithography,4 are methods of fabricating accurate, solid, 3D models from virtual data that can be used to replicate the patient’s bony anatomy. When interactive planning software is used, these manufacturing techniques can also be used to create surgical guides, directing drills to the positions of the planned implant osteotomies. Figure 1 shows an example of a sophisticated surgical plan that depicts bony topography, vital structures, ideal implant positions, guide stabilization pins, and the restorative design all on the same image.
Surgical guides can be fabricated to seat on teeth, soft tissue, or bone.5 Those that fit on bone frequently require significant flap elevation for surgical exposure of enough alveolar surface to create a precise stable fit. Bone-supported guides cannot be used for flapless surgery. It may be challenging to design this kind of guide when teeth are to be extracted in the surgical field. Data for these guides can be read from the diagnostic scan without additional diagnostic casts or intraoral imaging.
Tooth-supported guides require that an adequate number of stable teeth are available to support the guide. When teeth are relatively far from the anticipated surgical site, movement, distortion, or displacement of the guide can occur, reducing its accuracy. Tooth-supported guides may be used with either flapless or traditional surgical procedures.
Tissue-supported guides seat on mucosal surfaces, potentially building in some inaccuracies due to the possibility for tissue compression or movement. Often these guides are designed to be stabilized using transverse locking screws or pins to prevent movement once the guide is inserted in the patient’s mouth (Figure 2).
There are currently no data to compare the accuracy of systems based on manufacturer or type of guide support. In a systematic review, Jung et al6 noted a mean accuracy of 0.74 mm at the entry point and 0.85 mm at the apex for a variety of guides and systems. However, the range of error was clinically significant, with maximum deviations reported of 4.5 mm at the entry point and 7.1 mm at the apex. Other accuracy studies7,8 noted similar results with various methods of template production, support, and stabilization.
Surgical guides are often recommended when flapless or minimally invasive procedures are performed, because visible landmarks are obscured by tissue and structures. It is generally accepted that minimally invasive implant surgery has some potential advantages over traditional flap procedures,9 including less postoperative pain. Surgical guides, whether CAD/CAM or laboratory-fabricated, have some drawbacks. They have some bulk, which may interfere with surgical procedures. They could impede flap reflection and surgical visualization. Computer-generated guides have embedded metal sleeves that closely match the diameter of the drills to be inserted through them. Irrigation cooling of the drills could be impeded, leading to overheating bone and healing complications. Additionally, the sleeves typically require the use of relatively long drills, creating potential inter-arch space problems.10
For both tooth- and tissue-supported guides, there is a requirement that the patient’s oral anatomy (teeth and/or alveolar contours) be merged with the virtually planned osteotomy positions. This can be done by sending the patient’s casts to the guide manufacturer, scanning a cast with a CBCT, or combining data from an intraoral optical scanner. This information is then merged with the CBCT digital imaging and communications in medicine (DICOM) data, creating a composite of radiographic and topographical (oral hard and soft tissue) data to be used for virtual planning, guide, or even restoration fabrication. With proper planning and rapid prototyping manufacturing software, a virtual wax-up, implant position, abutment design, surgical guide, provisional restoration, and final restoration could all be planned and fabricated digitally. Even alveolectomy, alveoplasty, implant position, and provisional restorations can be anticipated, guided, and planned with these techniques.11
Prefabricating restorations using digital planning, guided surgery, and rapid prototyping or milling is possible but has not become routine due to various difficulties and limitations. Several authors12-15 describe different methods and systems to create these restorations. While preoperative analysis, planning, and preparations for these respective systems are complex and time-consuming, they appear to provide accurate, minimally invasive, and predictable results.
Prerequisite to prefabricating immediate restorations is the ability to precisely control implant depth and rotational orientation from planning through surgical placement. Surgical guides produced with rapid prototyping techniques can be designed either for drilling the osteotomies (partially guided) or additionally for placing the implants (totally guided).16 An increasing number of systems offer the option of total guidance, which also requires special surgical instruments for implant placement.
Another technology being developed for implant planning and surgery is surgical navigation.17 Used in orthopedics, neurosurgery, and ENT surgery, this technology uses visual or tactile feedback to communicate the desired implant position to the surgeon rather than a rigid guide (Figure 3). The computer is “connected” to the patient and the drill, and displays or directs the drill in real-time relative to the planned position.
As with any new technology, a learning curve is associated with implementing image guidance into practice. All patients to be treated with image guidance require a computerized scan, most likely CBCT. The data is exported into planning software where the dentist can analyze bony anatomy relative to the planned restoration, identify vital structures, and place virtual implants. Some planning software requires the user to convert the CBCT data into a proprietary format, termed reformatting, before analysis. Others directly use the DICOM files generated by the CBCT.
Analysis and planning of a case should become a collaborative process with the restorative dentist, surgeon, and patient. Decisions on implant number, position, angulation, grafting requirements, and surgical risk assessment can be made. While some radiology services offer implant planning as part of their service, the final responsibility for the accuracy and integrity of the plan rests with the treating dentists and cannot be delegated.
Incorporating image guidance into implant practice offers many advantages for the treatment team as well as patients. The greatest value is that preoperative planning rather than intraoperative mental navigation drives treatment. This can give the treatment team adequate time and accurate, intuitive tools for case planning to achieve superior, consistent results. Compromises, modifications, alterations, and cost considerations can be evaluated, discussed, and negotiated before initiating treatment. This reduces aggravation, complications, and misunderstandings. Future applications will facilitate faster, more comfortable, and more predictable implant dentistry, including more accurate diagnosis, minimally invasive surgery, immediate restoration/loading, and reduced treatment time.
Lastly, CT-based image guidance cannot be considered a substitute for adequate training, sound clinical judgment, experience, or expertise. Technology cannot usurp biology, no matter how sophisticated these systems become.
1. Rosenfeld AL, Mandelaris GA, Tardieu PB. Prosthetically directed implant placement using computer software to ensure precise placement and predictable prosthetic outcomes. Part 1: diagnostics, imaging, and collaborative accountability . Int J Periodontics Restorative Dent. 2006;26(3):215-221.
2. Kopp KC, Koslow AH, Abdo OS. Predictable implant placement with a diagnostic/surgical template and advanced radiographic imaging . J Prosthet Dent. 2003;89(6):611-615.
3. Popat AH. Rapid prototyping and medical modeling. Phidias Newsletter. Denmark; 1998;1:10-12
4. Laney WR, ed. Glossary of Oral and Maxillofacial Implants. Chicago, IL. Quintessence Publishing; 2007.
5. Mandelaris GA, Rosenfeld AL. Surgiguide Options. In: Tardieu PB, Rosenfeld AL, eds. The Art of Computer-Guided Implantology. Chicago, IL: Quintessence Publishing; 2009:67-88.
6. Jung RE, Schneider D, Ganeles J, et al. Computer technology applications in implant dentistry: a systematic review . Int J Oral Maxillofac Implants. 2009;24(suppl):92-109.
7. Schneider D, Marquardt P, Zwahlen M, Jung RE. A systematic review on the accuracy and the clinical outcome of computer-guided template-based implant dentistry . Clin Oral Implants Res. 2009;20(suppl 4):73-86.
8. Valente F, Schiroli G, Sbrenna A. Accuracy of computer-aided oral implant surgery: a clinical and radiographic study . Int J Oral Maxillofac Implants. 2009;24(2):234-242.
9. Fortin T, Bosson JL, Isidori M, Blanchet E. Effect of flapless surgery on pain experienced in implant placement using an image-guided system . Int J Oral Maxillofac Implants. 2006;21(2):298-304.
10. Ganeles J, Grossberg D. Complications related to immediately loaded dental implants. In: Froum SJ, ed. Dental Implant Complications: Etiology, Prevention, and Treatment. Ames, Iowa: Wiley-Blackwell; 2010;356-377.
11. Balshi SF, Wolfinger GJ, Balshi TJ. A protocol for immediate placement of a prefabricated screw-retained provisional prosthesis using computed tomography and guided surgery and incorporating planned alveoplasty . Int J Periodontics Restorative Dent. 2011;31(1):49-55.
12. Rosenfeld AL, Mandelaris GA, Tardieu PB. Prosthetically directed implant placement using computer software to ensure precise placement and predictable prosthetic outcomes. Part 3: stereolithographic drilling guides that do not require bone exposure and the immediate delivery of teeth . Int J Periodontics Restorative Dent. 2006;26(5):493-499.
13. Sanna AM, Molly L, van Steenberghe D. Immediately loaded CAD-CAM manufactured fixed complete dentures using flapless implant placement procedures: a cohort study of consecutive patients . J Prosthet Dent. 2007;97(6):331-339.
14. Tahmaseb A, De Clerck R, Wismeijer D. Computer-guided implant placement: 3D planning software, fixed intraoral reference points, and CAD/CAM technology. A case report . Int J Oral Maxillofac Implants. 2009;24(3):541-546.
15. Tahmaseb A, De Clerck RD, Eckert S, Wismeijer D. Reference-based digital concept to restore partially edentulous patients following an immediate loading protocol: a pilot study . Int J Oral Maxillofac Implants. 2011;26(4):707-717.
16. Mandelaris GA, Rosenbeld AL, King SD, Nevins ML. Computer-guided implant dentistry for precise implant placement: combining specialized stereolithographically generated drilling guides and surgical implant instrumentation . Int J Periodontics Restorative Dent. 2010;30(3):275-281.
17. Casap N, Tarazi E, Wexler A, et al. Intraoperative computerized navigation for flapless implant surgery and immediate loading in the edentulous mandible . Int J Oral Maxillofac Implants. 2005;20(1):92-98.
Jeffrey Ganeles, DMD
Assistant Clinical Professor, Periodontics
Nova Southeastern University
Ft. Lauderdale, Florida
Private Practice
Boca Raton, Florida
George A. Mandelaris, DDS, MS
Private Practice
Periodontics and Dental Implant Surgery
Park Ridge and Oakbrook Terrace, Illinois
Alan L. Rosenfeld, DDS
Clinical Professor, Graduate Periodontics
University of Illinois College of Dentistry
Chicago, Illinois
Private Practice
Periodontics and Dental Implant Surgery
Park Ridge and Oak Brook Terrace, Illinois