Newsletter
NewsletterDentists not using advanced radiology equipment are likely overexposing their patients and losing money.
By Dale Miles, DDS, MS
While most practitioners have already adopted computers with practice management systems and peripherals such as digital cameras, intraoral cameras, and even CAD/CAM devices, they may not yet realize that their X-ray system, too, can be easily integrated into this new digital world. By “upgrading” radiographic tools, they can make their work life easier and their practices more productive using technology that makes it possible to take extraoral bitewings and produce better data for clinical decisions such as implant planning. Radiology equipment is so advanced and the return on investment so rapid that those not using any of the technologies described are probably overexposing their patients and losing money at the same time.1
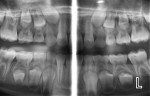
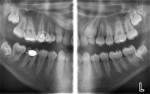
Some clinicians are not aware that they can take high-resolution (7-8 line pairs/mm) extraoral/panoramic bitewings. Dentists with pediatric patients may never have to put another image receptor in a child’s mouth again, and periodontists can take vertical bitewings without positioning problems. This is because several manufacturers now make panoramic machines that have bitewing programs. The disadvantage of the panoramic image for caries detection in the past has been inadequate line pair resolution and overlap of the contact points in the bicuspid regions. These deficiencies are now a thing of the past. One manufacturer (Planmeca, www.planmecausa.com) offers a patented technology called Selectively Compliant Articulating Robotic Arm (SCARA). The only machine to have a C arm on the top of its carriage, the bitewing acquisition is done robotically, with the patient in a typical panoramic position and the carriage moving inward toward the patient with a different start position to open contacts on most patients (Figure 1 through Figure 5). Of course, as with any dentition, if the tooth is ectopic or rotated, an additional image may be necessary to open the contacts. However, the quality of the image and ease of acquisition make this a very attractive technology. Looking carefully at the images, it is apparent that they are not only high-quality interproximal bitewing X-rays, but also high-quality periapical images from the canine to the molar region. Thus, with a digital panoramic machine capable of bitewing projections and producing excellent initial periapical views, the dose to the patient will be lower in most cases by eliminating unnecessary intraoral images. Although it is not a replacement technique, several dental schools in North America—including the Arizona School of Dentistry & Oral Health (ASDOH)—have adopted the protocol of using a panoramic and the extraoral panoramic bitewing/periapical projection as their initial radiographic examination. In addition, offices using this approach will find that there are fewer retakes and, therefore, less staff frustration related to radiographic procedures. At ASDOH, it has been found to reduce the number of full-mouth X-ray series, and intraoral and supplemental bitewing X-rays are needed only when indicated by selection criteria.
In addition to the possible reduction or even elimination of intraoral images for certain pediatric patients, the examples provided indicate that periodontists requiring vertical bitewings may also be interested in these contemporary panoramic machines.
Although dental schools have taught the use of rectangular collimation for more than 35 years, few dentists in private practice use this X-ray dose-reduction tool. This is mainly due to their belief that it would be difficult for dental assistants using this technology to “hit” the X-ray film; hence, the persistence of large, round cones on intraoral dental X-ray machines. The Food and Drug Administration, the National Council on Radiation Protection (NCRP), and the American Dental Association, all recommend the use of rectangular collimation for intraoral dental exposures. In fact, the latest guidelines from the NCRP report #145 state:
“Equipment designed for use with intraoral image receptors shall be capable of providing rectangular collimation to approximate the dimensions of the image receptor. The linear dimensions of the beam in each axis should not exceed those of the receptor by more than two percent of the source-to-image receptor distance. This collimation may be inherent in the x-ray machine position-indicating device.”
Several “low-tech” solutions have been introduced to the dental profession over the years. These are primarily devices that patients hold close to their face while the dental assistant or hygienist aims at the intraoral image receptor freestyle.
Another more “high-tech” device is one in which the receptor (film, phosphor plate, or solid-state) is fixed to an existing round cone by a rectangular adapter by magnets. This arrangement virtually eliminates stray radiation and “cone cuts.” Figure 6 shows a device called the Tru-Align® from Interactive Diagnostic Imaging, LLC (www.idixray.com), which virtually eliminates retakes—except those caused by placing the bite block on the wrong tooth—because the X-ray generator is physically linked to the position-indicating device and the patient.
No matter which rectangular collimating device is chosen, patients benefit from lower X-ray doses and clinicians can take comfort in knowing they are doing the best they can to protect their patients.
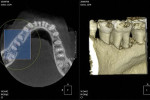
CBCT (cone beam computed tomography) is for everyone. It is not necessary to own one of these machines to use the data from it. CBCT data sets can be burned onto CD-ROMs or sent via the Internet to a dentist to open in third-party software such as implant-planning software or other viewing software. The impact of this technology has been rapid and universal.2-4 It is recommended that the general dentist use a “multifunctional” CBCT machine, one that can provide a conventional digital panoramic and other images and the software programs to create images such as those seen in this article, as well as cone beam information when desired or required.
Below is a partial list of panoramic machines capable of delivering a conventional 2-dimensional (2-D) panoramic image and 3-dimensional (3-D) cone beam CT. Note that many of these manufacturers have more than one “platform” for their 2-D/3-D machines.
• Carestream: 9300 (Carestream Health, Inc., www.carestream.com)
• J. Morita: Veraviewepocs® 3De (Morita USA, www.morita.com)
• Planmeca: ProMax (Planmeca®, www.planmecausa.com)
• Sirona: Orthophos XG 3D (Sirona, www.sirona.com)
• Soredex: Cranex® 3D (Soredex, www.soredex.com)
• Vatech: PaX-Duo 3D (Vatech, www.vatechamerica.com)
It is the author’s opinion that “multifunctional” panoramic/CBCT machines are the most appropriate and the most cost-effective imaging devices for the general practitioner. Small-volume (small-FOV) CBCT machines require less “re-education” for the dentist because there is slightly less anatomy to rediscover and interpret. If you purchase a panoramic machine with CBCT capability, the panoramic and specialized panoramic images accelerate the ROI for the CBCT functions. With proper examination of the patient and the selection of the appropriate modality—panoramic, panoramic bitewing, and/or CBCT—your clinical decisions will be made more easily and more accurately, and your patient will benefit from more precise treatment.
The author is a consultant for PlanmecaUSA; receives material support from CyberMed International; and is part owner of Interactive Diagnostic Imaging.
1. McKenzie S. Digital radiography ROI: Above the bottom line. Dental Compare. 2008:December. Available at: http://www.dentalcompare.com/Featured-Articles/2045-Digital-Radiography-ROI-Above-the-Bottom-Line/.
2. Miles DA, Danforth RA. A clinician’s guide to understanding cone beam volumetric imaging. Academy of Dental Therapeutics and Stomatology. 2007;Special I ssue:1-13.
3. Miles DA. The agony and the ecstasy of buying cone beam technology. Part I—The Ecstasy. JIACD. 2009;1(1):19-31. Available at: http://www.nxtbook.com/nxtbooks/specops/jiacd_200903/#/20.
4. Miles DA. Color Atlas of Cone Beam CT for Dental Applications (title change). 2nd ed. Quintessence Publishing Company, Inc., Hanover Park, IL: September 2012, in press.
Dale Miles, DDS, MS
Chief Executive Officer
Digital Radiographic Solutions
Fountain Hills, Arizona
Private Practice
Fountain Hills, Arizona
Vice President of Research
Interactive Diagnostic Imaging
Atlanta, Georgia